If you are soaking through a pad every hour, setting alarms at night to change protection, or passing clots the size of a coin — you are not being dramatic. Heavy periods are a medical issue, not something you just have to put up with. They have a name (menorrhagia), they have causes, and most of those causes have real solutions.
Here are the 9 most common reasons your period is heavier than it should be — explained clearly, with exactly what helps each one. Save this page. You will want to come back to it.
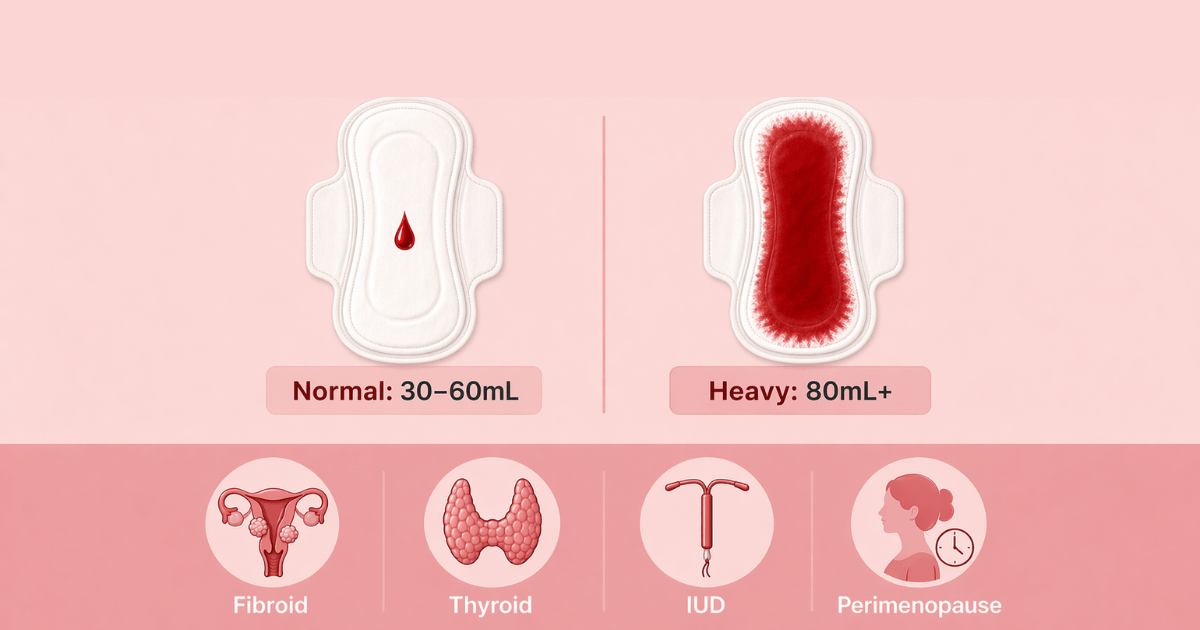
How Heavy Is "Too Heavy"?
Doctors define heavy menstrual bleeding (menorrhagia) as losing more than 80mL of blood per cycle. You don't need to measure it. Instead, use these signs:
- You soak through a full pad or tampon in under an hour — for several hours in a row
- You need to double up (pad + tampon simultaneously)
- You pass clots larger than a 50p coin or a US quarter
- Your period lasts longer than 7 days
- You feel dizzy, exhausted, or breathless during your period
- Heavy flow stops you working, exercising, or sleeping normally
If two or more of those apply to you — keep reading. And then book a doctor's appointment, because you deserve an answer.
1. Uterine Fibroids — The Most Common Cause
Fibroids are benign (non-cancerous) muscle growths inside or on the wall of the uterus. They affect up to 70% of women by age 50, and most never cause any problems. But fibroids that grow inside the uterine cavity — called submucosal fibroids — are one of the leading causes of extremely heavy periods.
Here's why: fibroids increase the surface area of the uterine lining that sheds during menstruation. More surface area = more bleeding. They also disrupt the normal blood vessel architecture of the uterus, making it harder to control blood loss naturally during a period.
Tell-tale signs alongside heavy flow: pelvic pressure or fullness, a feeling of bloating or that your uterus is enlarged, needing to urinate frequently, or pain during sex.
What helps: Hormonal IUD (reduces bleeding by 80–90% even with fibroids), tranexamic acid, GnRH agonists to shrink fibroids temporarily, or surgical options (myomectomy to remove fibroids, or hysterectomy in severe cases). Diagnosis is via pelvic ultrasound.
2. Adenomyosis — The Under-Diagnosed Culprit
Adenomyosis is a condition where the tissue that normally lines the uterus (endometrium) grows into the muscular wall of the uterus itself. The result is a uterus that is boggy, enlarged, and — when it sheds — does so heavily and painfully.
It affects an estimated 10–35% of women, yet takes an average of 8–12 years to diagnose because its symptoms overlap with fibroids, endometriosis, and "just bad periods." If your heavy period is also extremely painful — cramping that feels more like labour than regular period pain — adenomyosis is worth investigating.
What helps: Hormonal IUD is often first-line and works well for many women. Anti-inflammatory medications (NSAIDs) reduce pain and flow. In severe cases not responsive to hormonal treatment, hysterectomy is curative. Diagnosis is via MRI or sometimes suspected on ultrasound.
3. Hormonal Imbalance — Estrogen Dominance
Your uterine lining (endometrium) grows under the influence of estrogen. Progesterone — produced after ovulation — counterbalances estrogen and keeps the lining from over-thickening. When progesterone is relatively low compared to estrogen (a state often called estrogen dominance), the lining builds up more than usual and sheds more heavily.
This can happen when:
- Ovulation is irregular or absent (meaning less progesterone is produced)
- Stress or poor sleep chronically suppress progesterone production
- Body fat is high (adipose tissue synthesises extra estrogen)
- Perimenopause causes more anovulatory cycles
What helps: Addressing the root cause — improving sleep, managing stress, supporting ovulation. Progesterone supplementation (prescribed by a doctor) in the luteal phase can directly reduce lining build-up. Hormonal IUD delivers localised progesterone directly to the uterus.
4. Thyroid Dysfunction
Your thyroid is involved in almost every aspect of your metabolism — including menstrual regulation. Hypothyroidism (underactive thyroid) is a particularly common and often missed cause of heavy periods. Thyroid hormones influence how the uterus contracts during menstruation and how blood clotting factors are produced.
When thyroid hormone levels are low, the uterus contracts less efficiently during menstruation (so blood loss is higher), and clotting factor production can be impaired (so bleeding takes longer to stop). The result is a heavier, longer period.
Look for other hypothyroid signs alongside your heavy period: fatigue that sleep doesn't fix, unexpected weight gain, hair thinning, feeling cold all the time, dry skin, brain fog, constipation.
What helps: A simple TSH blood test confirms hypothyroidism. Levothyroxine (synthetic thyroid hormone) is highly effective — and many women find their periods normalise within 1–2 cycles of starting treatment.
5. Copper IUD
The copper IUD is a highly effective, hormone-free contraceptive — but it comes with a well-documented side effect: periods that are significantly heavier and more crampy, particularly in the first 3–6 months after insertion.
Copper ions in the uterine cavity trigger a local inflammatory response that increases prostaglandin production. Prostaglandins drive uterine contractions and affect blood vessel dilation during menstruation — both of which increase blood loss. Studies show copper IUD users lose approximately 20–50% more blood per cycle compared to pre-insertion.
What helps: NSAIDs (ibuprofen, mefenamic acid) taken from the day before your period starts reduces prostaglandin-driven blood loss by 25–35%. Tranexamic acid helps on the heaviest days. For most women, the heaviness reduces somewhat after 6 months as the uterus adjusts. If it remains unmanageable after 6–12 months, switching to a hormonal IUD may suit you better.
6. PCOS
PCOS is most commonly associated with infrequent or absent periods — but when periods do arrive in women with PCOS, they can be extremely heavy. Here's why: because ovulation is irregular, the uterine lining is not shed at the usual 28–35 day intervals. Instead, it builds up over a longer period under continued estrogen exposure, without the normal progesterone-mediated regulation.
When shedding finally occurs, there is more lining to lose — often producing a heavy, prolonged bleed that may be accompanied by large clots. Some women with PCOS describe their periods as "floodgates opening."
What helps: Regulating the cycle with hormonal treatment (combined pill, hormonal IUD, or cyclic progesterone) prevents the lining from over-building. Addressing the underlying insulin resistance driving PCOS — through dietary changes, weight management where appropriate, or metformin — can restore more regular ovulation over time.
7. Endometrial Polyps
Endometrial polyps are small, soft growths that develop on the inner wall of the uterus. They are almost always benign and very common — affecting up to 10% of women across all age groups. Even a single small polyp can cause noticeably heavier periods and bleeding between periods because it disrupts the normal, clean shedding of the uterine lining.
Polyps are usually discovered incidentally on a pelvic ultrasound or during investigation for heavy or irregular bleeding. They are easily removed via hysteroscopy (a minimally invasive procedure using a thin camera inserted through the cervix) — and removal typically resolves the abnormal bleeding immediately.
What helps: Hysteroscopic polypectomy is the definitive treatment. If you have heavy periods and your ultrasound shows a thickened or irregular endometrium, polyps may be the explanation.
8. Clotting Disorders — More Common Than You Think
This one surprises many people: von Willebrand disease — an inherited clotting disorder — affects approximately 1% of the general population and is significantly under-diagnosed in women because its primary symptom is heavy menstrual bleeding.
In normal menstruation, blood vessels in the shedding endometrium seal themselves via platelet plugs and clotting factors. In women with von Willebrand disease or other platelet function disorders, this sealing process is impaired — so bleeding continues longer than it should.
Consider a clotting disorder if you also have a history of: nosebleeds that take a long time to stop, easy bruising, prolonged bleeding after dental work, cuts that bleed longer than expected, or a family history of heavy bleeding.
What helps: Diagnosis requires specific blood tests (von Willebrand factor antigen and activity levels, ristocetin cofactor activity) — a standard clotting screen will not detect it. Treatment options include tranexamic acid, hormonal methods, or desmopressin (DDAVP) — a medication that temporarily raises von Willebrand factor levels.
9. Perimenopause
In the years approaching menopause — typically from the mid-40s, though sometimes earlier — cycles become less regular, and periods often become heavier before eventually tapering off. As ovarian function fluctuates, estrogen levels spike unpredictably while progesterone production declines. This hormonal volatility causes the uterine lining to build up unevenly and shed heavily.
If you are in your 40s and your periods have become noticeably heavier over the past year — especially if accompanied by cycle irregularity, hot flushes, night sweats, or mood changes — perimenopausal hormonal changes are a likely contributor.
What helps: Hormonal IUD is often the most effective option — it reduces bleeding while also providing contraception (which is still needed in perimenopause). Combined HRT or cyclical progesterone can also stabilise the lining. A FSH blood test can help confirm perimenopause.
Log Your Flow — See Your Pattern
Tracking how heavy your period is each day gives you data that makes a real difference at a doctor's appointment. Wamiga lets you log flow intensity, clots, pain, and symptoms cycle by cycle — so you arrive with a clear picture, not just a feeling. Free on iOS and Android.
What Actually Helps — Quick Reference
- Ibuprofen / Mefenamic acid (NSAIDs): Reduces flow by 25–35%. Take from the day before your period starts. Available over the counter. Works for most causes.
- Tranexamic acid: Reduces flow by up to 50%. Prescription only. Taken only on heavy days — it helps blood clot more effectively. Not a contraceptive, not hormonal.
- Hormonal IUD (Mirena): Reduces flow by 80–90% in most women within 3–6 months. Works for fibroids, adenomyosis, PCOS, estrogen dominance, perimenopause. Highly effective long-term solution.
- Combined pill: Regulates the cycle, controls lining build-up, reduces flow by around 40–50%.
- Cyclic progesterone: Useful when hormonal contraception is not wanted. Progesterone in the second half of the cycle prevents lining over-thickening.
- Iron supplementation: Does not reduce blood loss, but essential if heavy periods have left you iron-depleted. Get a ferritin test.
- Surgery: For fibroids (myomectomy), polyps (hysteroscopic removal), adenomyosis (hysterectomy in severe cases). Reserved for when medical management fails.
Don't Ignore Your Iron
This is one of the most overlooked consequences of heavy periods, and it quietly affects millions of women.
Repeated heavy periods deplete iron stores faster than the body can replace them through diet alone. Low iron means less haemoglobin — the protein in red blood cells that carries oxygen. The result: fatigue that no amount of sleep fixes, breathlessness climbing stairs, feeling cold, difficulty concentrating, hair loss, and a general sense of running on empty.
Many women living with these symptoms assume it's just life — stress, being busy, not sleeping enough. Often, it's iron.
Ask your doctor for a serum ferritin test (stored iron), not just a standard haemoglobin check. Ferritin below 30 ng/mL is considered low even if your haemoglobin looks normal — and symptoms of deficiency typically appear well before anaemia is diagnosable. If your ferritin is low, an iron supplement (ferrous sulfate or ferrous bisglycinate) alongside dietary iron (red meat, lentils, leafy greens with vitamin C) can restore levels within 8–12 weeks.
Frequently Asked Questions
What is considered a heavy period?
Medically: more than 80mL of blood per cycle. Practically: soaking a pad or tampon in under an hour for several hours in a row, needing to double up on protection, passing clots larger than a 50p coin or quarter, bleeding for longer than 7 days, or flow that significantly disrupts daily life. Two or more of these signs means your period is worth discussing with a doctor.
What causes a suddenly heavy period?
A sudden increase in heaviness is most commonly caused by uterine fibroids, a newly fitted copper IUD, a hormonal shift (declining progesterone relative to estrogen), thyroid dysfunction, or the early stages of perimenopause. If your period has become noticeably heavier over 2–3 cycles with no obvious cause, a pelvic ultrasound and hormone blood panel can usually identify it.
Can a heavy period be a sign of something serious?
Most heavy periods are caused by benign conditions — fibroids, adenomyosis, hormonal imbalance, or a copper IUD. Rarely, heavy bleeding can indicate endometrial hyperplasia or endometrial cancer, particularly in women over 45 or with long-standing irregular cycles from PCOS. Any heavy bleeding accompanied by pain between periods or postmenopausal bleeding warrants prompt evaluation.
What is the fastest way to reduce a heavy period?
Ibuprofen (400–600mg every 6–8 hours, taken from the day before your period) reduces flow by 25–35% by lowering prostaglandins. Tranexamic acid (prescription) reduces flow by up to 50% on the heaviest days. These don't cure the cause but make the current cycle manageable while you investigate with a doctor.
Does a heavy period mean low iron?
Repeated heavy periods are one of the leading causes of iron deficiency in women of reproductive age. If you feel persistently tired, breathless, cold, or foggy around your period, get a serum ferritin test — stored iron can be depleted well before a standard blood test shows anaemia. Many women with heavy periods benefit from an iron supplement regardless of whether full anaemia is present.