Period Health
Period Back Pain: Why It Happens and How to Relieve It
Prostaglandins and referred nerve pathways explain why your uterus makes your back ache — and 7 proven relief methods.
That pounding head every time your period arrives is not random — it's driven by a predictable hormonal chain reaction. Here's the science behind period headaches and 7 evidence-based ways to stop them.

You notice the headache arriving like clockwork — two days before your period or the moment it starts. It's not stress. It's not a bad night's sleep. It's hormones, and it follows a script your body has been running for years. If this sounds familiar, you're in very good company: 60% of women who experience migraines identify their menstrual cycle as a trigger, according to the National Headache Foundation.
Period headaches range from a dull, pressure-like ache that sits behind your eyes all day to a full menstrual migraine that sends you to a dark room for 72 hours. Understanding which type you have — and why it's happening — is the first step to actually preventing it.
"Period headache" is an umbrella term that covers any headache occurring in the days before, during, or just after menstruation. Doctors classify them into two clinical subtypes based on the International Classification of Headache Disorders (ICHD-3):
| Type | When It Occurs | Prevalence | Key Feature |
|---|---|---|---|
| Pure Menstrual Migraine (PMM) | Day −2 to +3 only, in ≥2 of 3 cycles. No attacks at other times. | 7–14% of all women | Attacks are exclusively cycle-linked |
| Menstrual-Related Migraine (MRM) | Day −2 to +3 in ≥2 of 3 cycles, but also occurs at other times | 35–54% of female migraineurs | Period makes existing migraines worse and more frequent |
| PMS Tension Headache | Premenstrual phase (days −7 to −1) | Very common, less studied | Dull bilateral pressure, less severe than migraine |
The distinction matters because menstrual migraines require different treatment strategies than simple tension headaches — particularly when it comes to prevention.
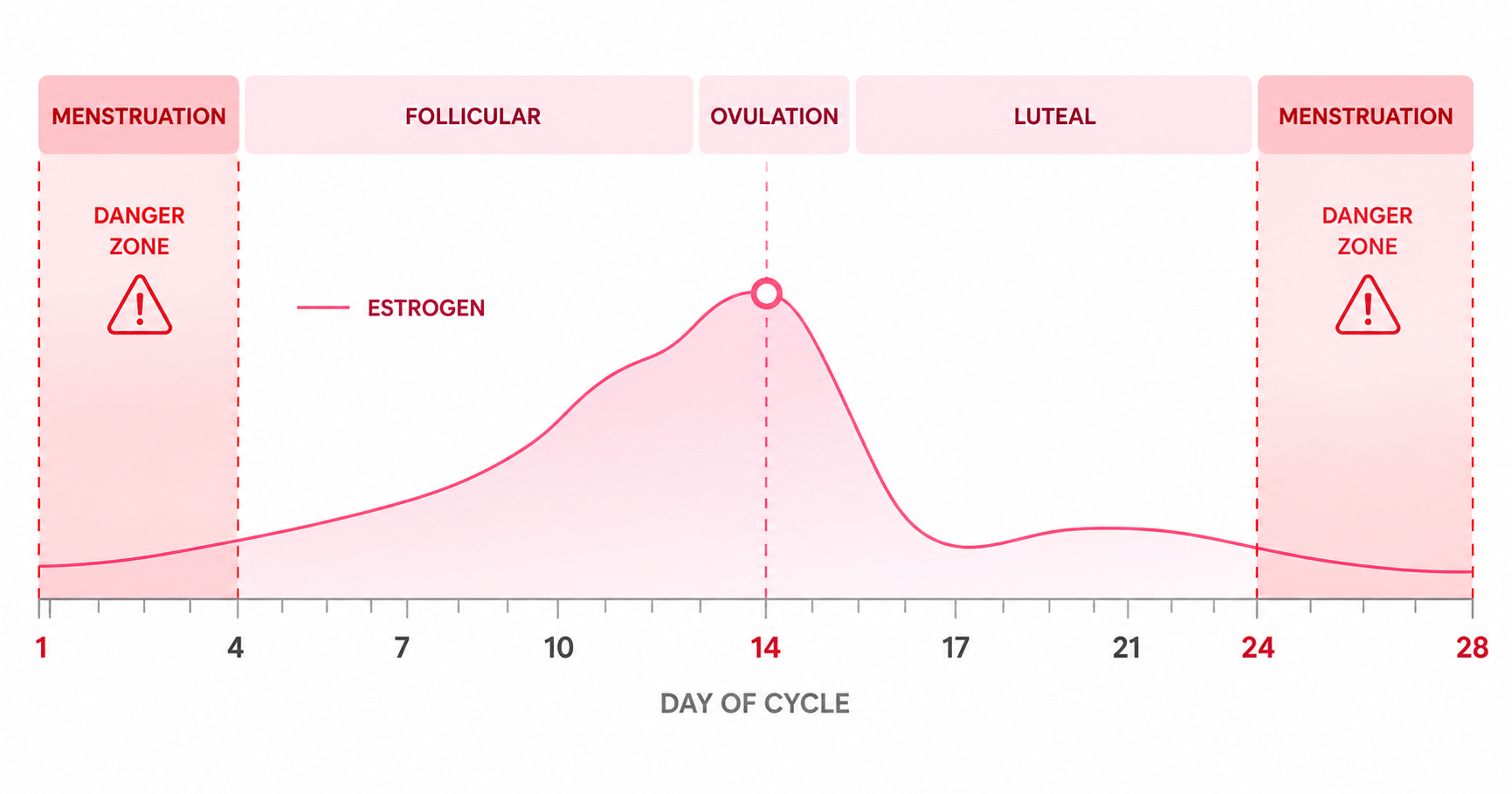
The trigger is estrogen withdrawal — the sharp fall in estrogen that happens in the 2–3 days before your period begins. Throughout your cycle, estrogen rises to support ovulation, then rises again in the luteal phase before dropping steeply in the days just before bleeding. It is this drop — not a constantly low estrogen level — that triggers the headache.
Here's why: estrogen regulates serotonin production and receptor sensitivity. When estrogen falls, serotonin levels fall with it. Low serotonin causes blood vessels in the brain to constrict and then dilate in a wave — producing the characteristic throbbing, pulsating pain of a migraine. Prostaglandins released during menstruation add a second pain layer by sensitising nerve endings throughout the body, including those in the head.
The two red danger zones are days 26–28 (estrogen crashes before bleeding starts) and days 1–2 of your period (risk is highest — you are statistically twice as likely to get a migraine on day 1 than on any other day of your cycle). By contrast, the follicular phase after your period, when estrogen is rising steadily, is typically your lowest-headache time of the month.
Not all period headaches are migraines — and telling them apart changes what you should reach for. A tension headache responds well to rest and basic pain relief. A true menstrual migraine often needs a triptan, not just ibuprofen.
If you feel like your period migraines are harder to shake than migraines you get at other times — you're right, and this is clinically documented. A within-woman study published in Neurology compared migraine attacks in the same women at different cycle phases and found that period-linked attacks are objectively more severe across every measure:
The reason comes back to biology. During menstruation, your body is simultaneously dealing with estrogen withdrawal AND a flood of prostaglandins causing uterine contractions. Both pathways sensitise pain receptors — so the migraine threshold is lower and the pain, once triggered, is harder to extinguish.
Estrogen withdrawal sets the scene, but these six factors act as accelerators — each one independently raises your migraine risk, and they often stack during the same 48-hour window.
The primary trigger — a 40–50% drop in estrogen in the 2–3 days before bleeding activates serotonin and vascular changes that fire the migraine cascade.
Released as the uterine lining sheds, prostaglandins cause systemic inflammation and sensitise pain receptors throughout the body — lowering your headache threshold further.
Estrogen helps retain magnesium. When it drops, so does your magnesium. Low magnesium promotes cortical spreading depression — the brain wave that underlies migraine.
Hormonal fluctuations around your period often disturb sleep quality. Poor sleep is one of the most reliably documented migraine triggers — independently of hormones.
PMS-related cortisol spikes and emotional stress directly raise neurological excitability and lower the pain threshold — amplifying an already sensitive system.
Many women reduce food and water intake during painful periods, or lose appetite. Both dehydration and hypoglycaemia are independent migraine triggers that compound the hormonal effect.
Track your headaches with Wamiga
Log headache days, severity, and cycle data all in one place. Tracking is the only way to clinically confirm a menstrual migraine — Wamiga makes that easy and automatic.
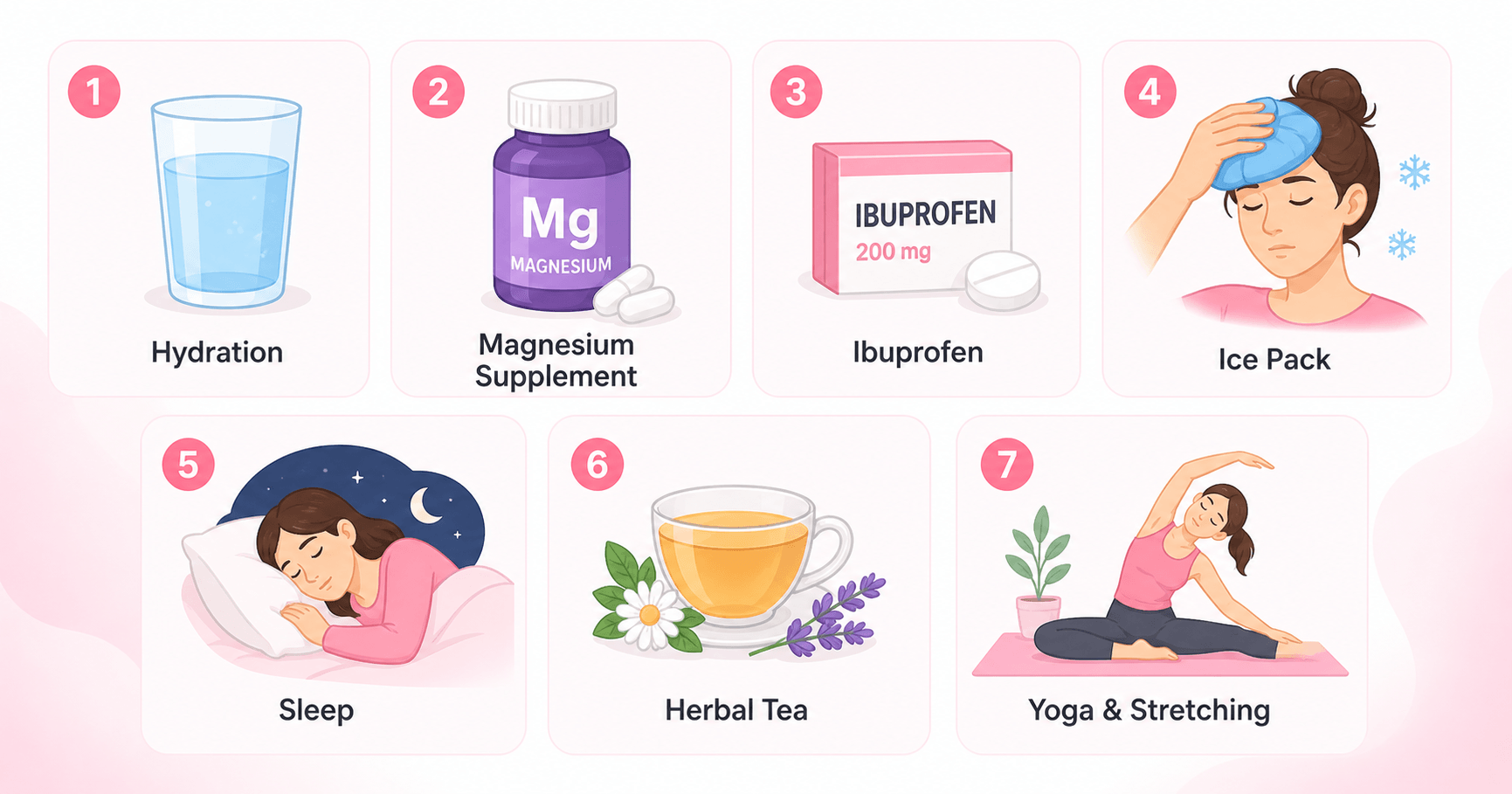
These methods are ranked loosely by evidence strength. The most important distinction is timing — for menstrual migraines specifically, starting treatment before the headache hits is far more effective than waiting.
For women whose menstrual migraines are severe or predictable, doctors use mini-prevention — a short course of medication taken only during the 5–7 day vulnerable window (days −2 to +3) rather than daily throughout the month. This can include:
Most period headaches are benign and manageable. But certain patterns signal that something more complex is happening and requires professional evaluation.
If your migraines are predictable and cycle-linked, a gynaecologist or headache specialist can offer targeted mini-prevention strategies that dramatically reduce the frequency and severity — without daily medication. The key is bringing a headache diary that documents the timing relative to your cycle. A period tracking app like Wamiga makes this automatic.
Period headaches — whether a dull PMS tension ache or a full menstrual migraine — are driven by a predictable hormonal mechanism: estrogen withdrawal, serotonin dysregulation, and prostaglandin-fuelled inflammation. They are real, common, and highly treatable.
The most underused strategy is timing — starting naproxen or magnesium before the headache hits, not after. The most underused tool is tracking — knowing your exact vulnerable window so you can act on it. If you can show your doctor a 2–3 month log confirming attacks consistently occur on days −2 to +3, you qualify for mini-prevention strategies that can be transformative. Wamiga builds that log for you automatically.
The guidance in this article is informed by reputable medical and public-health organizations:
Prostaglandins and referred nerve pathways explain why your uterus makes your back ache — and 7 proven relief methods.
From ibuprofen to heat pads — 12 evidence-backed ways to beat period cramps quickly.

Bloating, cramps, mood changes and more — the 15 most common signs your period is on its way.