80–95%
Of menstruating women experience at least one PMS symptom — it is the most common hormonal complaint in reproductive health
25+
Clinically recognised PMS symptoms across physical, emotional, and behavioural categories
5–14 days
Before your period when symptoms appear — entirely during the luteal phase, and should resolve within days of bleeding starting
In this article
- What is PMS? (Quick definition)
- Physical PMS symptoms (14 signs)
- Emotional and behavioural symptoms (11 signs)
- When PMS symptoms appear in your cycle
- Why you get PMS: the hormonal science
- PMS vs pregnancy symptoms: key differences
- PMS vs PMDD: understanding the severity spectrum
- What actually relieves PMS symptoms (with evidence)
- When to see a doctor
- Frequently asked questions
What is PMS?
Premenstrual syndrome (PMS) is the collection of physical, emotional, and behavioural symptoms that occur in the luteal phase of the menstrual cycle — the 1–2 weeks between ovulation and menstruation — and resolve within a few days of bleeding starting. To meet the clinical definition set by the American College of Obstetricians and Gynecologists (ACOG), you need:
- At least one physical symptom and one emotional symptom
- Symptoms present in the 5 days before your period in each of three consecutive cycles
- Symptoms that resolve within 4 days of your period starting
- Symptoms that do not recur until at least cycle day 13
- Symptoms that cause some degree of impairment in normal functioning
Note that having one or two uncomfortable days before your period is not necessarily clinical PMS — most women experience some degree of premenstrual awareness. The clinical threshold is where symptoms reliably impair daily activities.
Physical PMS symptoms
Physical symptoms are driven by progesterone's systemic effects and the downstream hormonal changes of the luteal phase. They typically begin a few days after ovulation and intensify in the final week before your period.
Bloating & Water Retention
Progesterone stimulates aldosterone, causing sodium and fluid retention. The abdomen, face, and hands can feel puffy and heavier. Typically peaks 1–2 days before period.
~50% of womenBreast Tenderness & Swelling
High estrogen and progesterone in the luteal phase stimulate breast tissue, causing soreness, heaviness, and hypersensitivity. One of the earliest symptoms to appear after ovulation.
~45% of womenCramps & Abdominal Pain
Pre-menstrual prostaglandin production causes uterine contractions before and during bleeding. Unlike period cramps, pre-menstrual cramping can start 1–2 days before flow begins.
Very commonFatigue & Low Energy
Progesterone's thermogenic and sedative-like effects, combined with serotonin depletion and disrupted sleep quality, produce marked tiredness — even after a full night's sleep.
~57% of womenHeadaches & Migraines
The sharp estrogen drop in late luteal phase triggers migraines in susceptible women by affecting serotonin and causing blood vessel reactivity. "Menstrual migraines" peak in the 2 days before and first 2 days of the period.
CommonBack Pain & Muscle Aches
Prostaglandins cause referred pain to the lower back and thighs. Progesterone-induced ligament laxity and water retention can worsen joint and muscle discomfort throughout the body.
CommonFood Cravings
Serotonin depletion in the luteal phase drives the brain to seek tryptophan (found in carbohydrates) to restore serotonin. Magnesium deficiency (worsened by progesterone) specifically triggers chocolate cravings.
~85% of womenSleep Disturbances
Both insomnia and hypersomnia are reported. Elevated progesterone disrupts REM sleep; rising core body temperature (BBT effect) affects sleep onset. Poor sleep amplifies every other PMS symptom.
CommonNausea
Progesterone slows gastrointestinal motility and can trigger mild nausea, especially in the mornings of the late luteal phase. Resolves quickly after menstruation begins.
Moderate prevalenceDigestive Changes
Constipation or loose stools in the days before the period — prostaglandins affect bowel motility in both directions. Some women experience the "period runs" that continue into the first days of bleeding.
CommonAcne & Skin Changes
Progesterone stimulates sebum production and can cause pre-menstrual breakouts, typically around the chin, jawline, and cheeks. Skin may also feel oilier or more sensitive overall in the luteal phase.
Very commonTemporary Weight Gain
Fluid retention (not fat) can add 1–3 kg in the late luteal phase. This resolves fully within a day or two of the period starting as aldosterone drops and fluid is excreted.
CommonElevated Basal Body Temperature
Progesterone's thermogenic effect raises resting body temperature by 0.2–0.5°C throughout the luteal phase — this is how BBT charting confirms ovulation. Some women notice feeling warmer or experiencing mild night sweats.
Universal in ovulatory cyclesDizziness or Light-headedness
Estrogen and progesterone fluctuations affect blood pressure regulation and vestibular sensitivity. Some women experience mild dizziness, particularly when standing quickly, in the late luteal phase.
Less commonEmotional and behavioural PMS symptoms
The emotional symptoms of PMS are driven primarily by serotonin depletion — as estrogen drops in the luteal phase, serotonin availability decreases, affecting mood regulation, stress tolerance, and emotional reactivity. These symptoms are just as real and physiologically caused as the physical ones.
Mood Swings
Rapid, unpredictable shifts in emotional state — from fine to tearful, from calm to angry — in minutes. Driven by serotonin and dopamine instability in the late luteal phase.
~64% of womenIrritability & Short Temper
Disproportionate frustration with minor annoyances; lower threshold for anger. Serotonin depletion reduces the brain's ability to modulate emotional reactions, making small stressors feel overwhelming.
~60% of womenAnxiety & Tension
A pervasive sense of unease, being "on edge," or worried about nothing specific. Progesterone's metabolite allopregnanolone affects GABA receptors differently in some women, reducing the calming effect of this neurotransmitter.
~64% of womenLow Mood & Tearfulness
Unexplained sadness, feeling down without a clear reason, or crying more easily than usual. Serotonin's role in mood regulation means its pre-menstrual depletion directly causes depressive-type symptoms.
CommonBrain Fog & Poor Concentration
Difficulty focusing, forgetting words, or feeling mentally slow. Serotonin and dopamine depletion, combined with poor luteal-phase sleep quality, impair cognitive processing and working memory.
CommonSocial Withdrawal
Wanting to be alone, cancelling plans, or feeling disconnected from others. Low serotonin reduces motivation for social interaction; heightened emotional sensitivity makes social situations feel draining.
Moderate prevalenceReduced Libido
Decreased interest in sex during the late luteal phase is common and biologically logical — progesterone dominance, fatigue, bloating, and mood changes all contribute. Libido typically restores in the follicular phase.
CommonInsecurity & Sensitivity
Feeling more self-critical than usual, reading neutral comments as criticism, or feeling unusually vulnerable to rejection. This heightened sensitivity is driven by decreased serotonin and dopamine tone.
CommonFeeling Overwhelmed
Normal responsibilities feel unmanageable. The combination of cognitive impairment, fatigue, emotional dysregulation, and physical discomfort reduces coping capacity — tasks that are fine mid-cycle feel impossible pre-period.
CommonEmotional Eating & Appetite Changes
Binge eating, comfort eating, or drastically reduced appetite. The serotonin-carbohydrate connection means the brain actively seeks food to restore mood — this isn't weakness, it's neurochemistry.
Very commonIndecisiveness
Difficulty making even small decisions — what to eat, what to wear, what to prioritise. Reduced dopamine and serotonin impair the prefrontal cortex's executive function and decision-making capacity.
Moderate prevalenceYou don't need all of these symptoms to have PMS. Most women have a personal pattern — typically 4–8 symptoms that repeat consistently each cycle. Identifying your pattern is the first step to managing it effectively, which is exactly what cycle tracking enables.
When PMS symptoms appear in your cycle
All PMS symptoms are confined to the luteal phase — the second half of your cycle, from ovulation to menstruation. One of the most diagnostic features of PMS (and the primary way it differs from depression) is the existence of a symptom-free window after your period starts and before ovulation.
28-Day Cycle: PMS Symptom Timing and Intensity
Period
(Day 1–5)
(Day 1–5)
Follicular Phase
(Day 6–13) — SYMPTOM FREE
(Day 6–13) — SYMPTOM FREE
Ov.
Early Luteal
(Day 15–20)
(Day 15–20)
Late Luteal — PEAK PMS
(Day 21–28)
(Day 21–28)
Symptom Intensity by Phase
None
None
—
Mild–Moderate
Moderate–Severe
Symptom-free window (confirms PMS vs depression)
Symptoms may begin (early luteal)
Peak PMS symptoms (late luteal)
Symptoms resolve within 1–4 days of menstrual flow beginning as progesterone drops and serotonin begins to recover.
Key timing patterns to know:
- Day 15–19 (Early luteal): Some women notice breast tenderness and mild mood shifts as progesterone begins rising
- Day 20–24 (Mid luteal): Bloating, fatigue, food cravings, and sleep changes often appear here
- Day 25–28 (Late luteal): Emotional symptoms peak; cramping and headaches may begin; all symptoms typically at their worst in the final 2–3 days
- Day 1–2 of period: Most symptoms resolve rapidly as progesterone drops and prostaglandins drive the period
Why you get PMS: the hormonal science
PMS isn't caused by "too much" or "too little" hormones — women with PMS have normal hormone levels. The root cause is an abnormal sensitivity to normal hormonal fluctuations, particularly the fall of estrogen in the late luteal phase and its knock-on effects on brain chemistry.
Estrogen Drop → Serotonin Falls
Estrogen modulates serotonin receptors and serotonin transporter activity. As estrogen declines in the late luteal phase, serotonin availability in the brain decreases — directly causing mood swings, irritability, anxiety, low mood, brain fog, food cravings (the brain seeks carbs to restore serotonin), and sleep disruption.
Progesterone → Aldosterone → Bloating
Progesterone stimulates aldosterone, a hormone that causes the kidneys to retain sodium and water. This is why bloating and breast swelling appear in the luteal phase and resolve once progesterone drops at menstruation, releasing the retained fluid rapidly.
Progesterone → Magnesium Wasting
Progesterone promotes magnesium excretion by the kidneys. Lower magnesium levels in the luteal phase contribute to fatigue, muscle cramps, headaches, and — notably — chocolate cravings (chocolate is one of the richest dietary sources of magnesium). This is why magnesium supplementation specifically helps PMS.
Prostaglandins → Cramps & Pain
As the endometrial lining prepares to shed, it produces prostaglandins (inflammatory signalling molecules). These cause uterine muscle contractions (cramps), intestinal contractions (diarrhoea), blood vessel dilation (headaches), and general inflammatory pain — which is why NSAIDs (prostaglandin inhibitors) are so effective for period and pre-menstrual pain.
PMS vs pregnancy symptoms: key differences
Several PMS and early pregnancy symptoms overlap, causing genuine confusion in the 1–2 week wait after ovulation. The key clinical difference: PMS symptoms resolve when your period starts; pregnancy symptoms persist and intensify.
| Symptom | PMS | Early Pregnancy |
|---|---|---|
| Breast tenderness | Starts after ovulation, resolves with period | Starts after implantation, persists and worsens |
| Fatigue | Present but mild–moderate; resolves with period | Often extreme exhaustion; persists through first trimester |
| Mood changes | Irritability, low mood — resolves with period | Emotional sensitivity; doesn't resolve when period is "due" |
| Bloating | Water retention; resolves day 1–2 of period | Digestive bloating; persists through first trimester |
| Nausea | Mild nausea possible; not the dominant symptom | Often prominent morning sickness; absent in PMS |
| Cramping | Pre-period cramps begin 1–2 days before period | Implantation cramping possible (~6–10 DPO); lighter than period cramps |
| Food cravings | General carb/sweet cravings | Specific, intense aversions and cravings; smell sensitivity |
| Spotting | Possible light pre-period spotting | Implantation bleeding (~6–10 DPO) — lighter, shorter, pinkish |
| Resolution | Symptoms clear when period starts | Symptoms persist after expected period date |
If your symptoms continue or worsen after your period was due — and your period hasn't come — take a home pregnancy test. A urine test is reliably accurate 12–14 days after ovulation (not 14 days after your last period started, which is a common mistake in women with longer cycles).
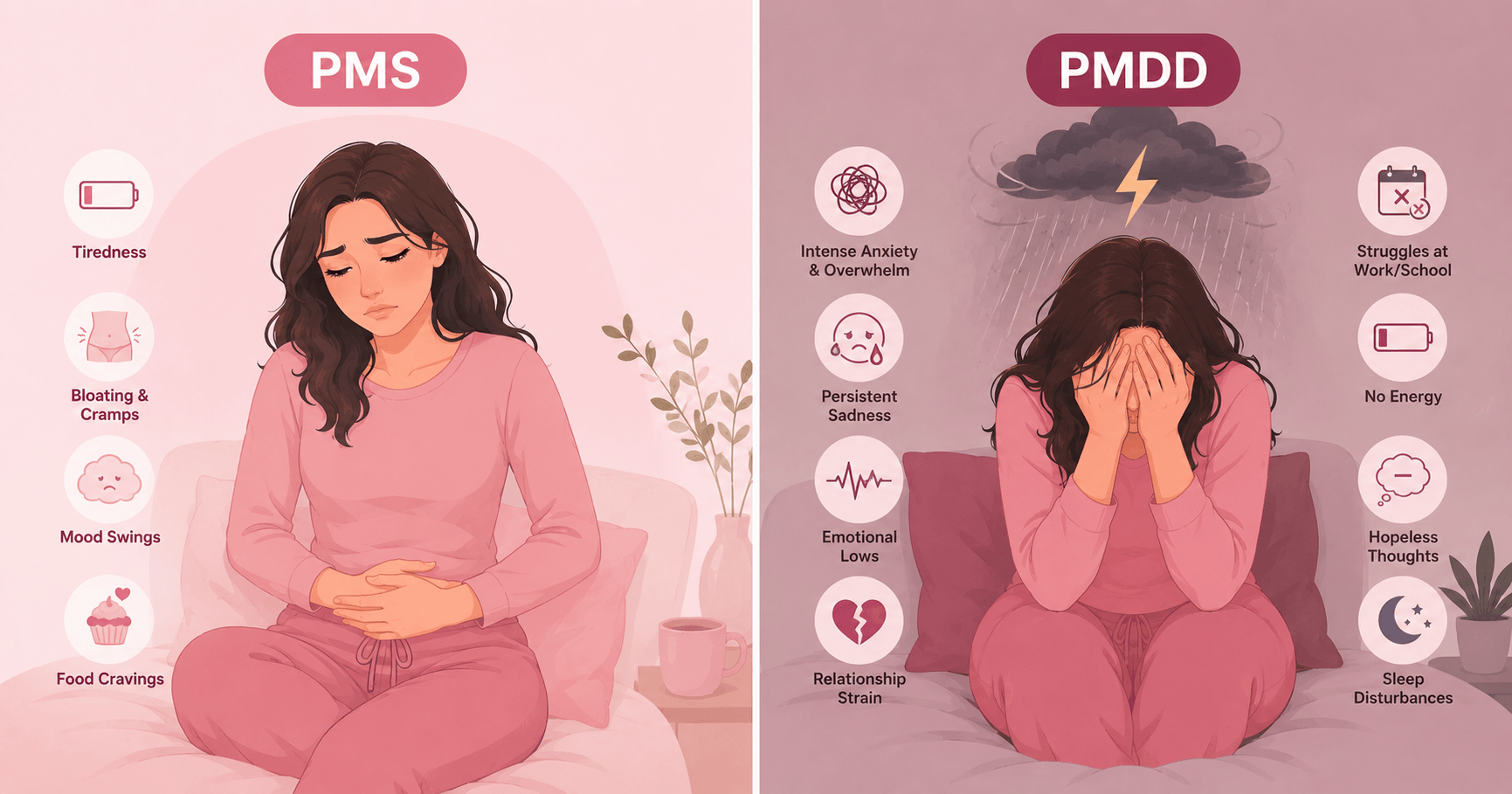
PMS vs PMDD: understanding the severity spectrum
PMS exists on a spectrum. The vast majority of women fall in the mild-to-moderate range; a smaller group experiences symptoms severe enough to warrant a clinical diagnosis of PMDD.
~50% of women
~30–40% of women
~3–8% of women
The line between severe PMS and PMDD is functional impairment. If your premenstrual symptoms are disrupting your work, ending or straining relationships, or causing thoughts of self-harm, that crosses into PMDD territory — a diagnosable condition with effective specific treatments. See our complete guide: PMS vs PMDD: How to Tell the Difference →
What actually relieves PMS symptoms
Here's the evidence-ranked breakdown — percentage estimates come from clinical trials and systematic reviews, not anecdote.
💊 NSAIDs (ibuprofen, naproxen) — for pain symptoms
60–70% relief Strong evidence
Start 1–2 days before pain symptoms typically begin. Most effective for cramps, back pain, and headaches by blocking prostaglandin synthesis. Available OTC.
🥛 Calcium — 1,200 mg/day (year-round)
~48% symptom reduction Strong evidence
RCT evidence (Thys-Jacobs et al.) shows calcium carbonate significantly reduces mood symptoms, bloating, pain, and food cravings. Benefits compound over 3 months. Take with Vitamin D for absorption.
🏃♀️ Aerobic exercise — 30 min, 5 days/week
30–50% reduction Strong evidence
The most well-supported lifestyle intervention. Exercise increases serotonin and endorphins, reduces cortisol, and improves sleep quality — targeting the root causes of both physical and emotional PMS. Must be consistent, not just in the luteal phase.
🌿 Magnesium — 360 mg/day during luteal phase
30–40% reduction Moderate evidence
Particularly effective for bloating, breast tenderness, mood symptoms, and headaches. Progesterone causes magnesium wasting, so replenishing it during the luteal phase addresses a genuine deficiency. Magnesium glycinate is better tolerated than oxide.
💡 Vitamin B6 — 50–100 mg/day
30–40% reduction (mood) Moderate evidence
B6 is a cofactor in serotonin and dopamine synthesis — directly addressing the neurotransmitter depletion driving emotional PMS. A Cochrane review found B6 twice as likely to relieve mood and depressive symptoms vs placebo. Don't exceed 100 mg/day long-term.
🧘 Reducing salt, caffeine & alcohol in luteal phase
20–30% reduction Moderate evidence
Salt worsens fluid retention and bloating. Caffeine amplifies anxiety and disrupts sleep. Alcohol depletes magnesium and disrupts serotonin metabolism — three things PMS already does. Reducing these in the 1–2 weeks before your period provides measurable relief.
💊 SSRIs — prescribed for significant mood symptoms
60–70% reduction Prescription
For moderate-to-severe emotional PMS and PMDD, SSRIs (fluoxetine, sertraline) are highly effective — and uniquely, can be taken only during the luteal phase (2 weeks before period) with equivalent efficacy to continuous dosing. Discuss with your doctor if lifestyle and supplement approaches haven't helped.
Tracking which symptoms you experience — and on which cycle days — helps you time remedies, identify patterns, and bring concrete data to your doctor. Wamiga lets you log symptoms daily alongside your cycle, turning weeks of data into a clear picture of your personal PMS pattern. Download Wamiga free →
When to see a doctor
Symptoms disrupt work or relationships
Missing days, making errors, or having significant conflicts specifically in the premenstrual phase — this meets the clinical threshold for treatment, not just lifestyle management.
Symptoms don't clear with your period
If physical or emotional symptoms persist beyond 3–4 days after your period starts, this may indicate a condition other than PMS — including depression, thyroid disorder, or endometriosis.
Thoughts of self-harm or suicidal ideation
Pre-menstrual suicidal thoughts are a recognised symptom of PMDD, not a character trait. Tell your doctor explicitly — this escalates the urgency and unlocks targeted treatment.
Symptoms are worsening over time
PMS that gets progressively worse with each cycle — especially after pregnancy, stopping birth control, or in your 30s–40s — deserves evaluation. It can be treated.
OTC remedies haven't helped after 3 months
If you've tried calcium, exercise, and ibuprofen consistently for 3 months without meaningful improvement, prescription options (SSRIs, hormonal contraceptives) are likely more appropriate for your severity.
You're unsure if it's PMS or something else
Several conditions mimic or overlap with PMS: depression, anxiety, endometriosis, PCOS, thyroid disorders. A doctor can rule these out with simple blood tests and a symptom diary review.
What to say at your appointment: Bring a 2-month symptom log showing dates, severity ratings, and cycle days. Say: "I've been tracking my symptoms and they consistently appear in the 1–2 weeks before my period and resolve when it starts. I'd like to discuss whether I have PMS or PMDD, and what treatment options are appropriate." Data always leads to better consultations.
Frequently asked questions
How many PMS symptoms are there?
Medical literature documents over 150 reported premenstrual symptoms, but clinically recognised PMS involves around 25–37 core symptoms grouped into physical and emotional/behavioural categories. The ACOG requires at least one physical and one emotional symptom present in the 5 days before your period across three consecutive cycles.
When do PMS symptoms start before your period?
PMS symptoms typically begin 5–14 days before menstruation — during the luteal phase. They usually peak in the final 2–3 days before the period starts and resolve within a day or two of menstrual flow beginning. Some women notice mild symptoms shortly after ovulation (~day 15), while others only notice symptoms in the final 3–5 days before their period.
What are the most common PMS symptoms?
Based on epidemiological studies, the most commonly reported PMS symptoms are: food cravings (~85%), mood swings and anxiety (~64%), irritability (~60%), fatigue (~57%), bloating and water retention (~50%), and breast tenderness (~45%). Individual patterns vary significantly.
Can PMS symptoms feel like pregnancy?
Yes — breast tenderness, fatigue, mood changes, bloating, and food cravings overlap significantly. The key differences: PMS symptoms resolve when your period starts; pregnancy symptoms persist and worsen. Nausea is more characteristic of pregnancy. A home pregnancy test taken 12–14 days after ovulation is the only reliable way to distinguish between them.
What causes PMS symptoms?
PMS is caused by abnormal sensitivity to normal luteal-phase hormonal fluctuations. The emotional symptoms are primarily driven by estrogen's drop reducing serotonin availability. Bloating is caused by progesterone stimulating aldosterone (fluid retention). Food cravings result from serotonin depletion plus progesterone-induced magnesium wasting. Pain comes from prostaglandin production as the endometrium prepares to shed.
What actually relieves PMS symptoms?
The treatments with the strongest evidence are: calcium (1,200 mg/day) reduces symptoms by ~48% in RCTs; regular aerobic exercise reduces symptoms by 30–50%; NSAIDs (ibuprofen, naproxen) relieve cramps and headaches by 60–70%. Magnesium (360 mg/day in the luteal phase) helps bloating and mood. For severe PMS, SSRIs prescribed by a doctor are highly effective.
When should I see a doctor about PMS?
See a doctor if: symptoms significantly disrupt your work, relationships, or daily functioning; symptoms don't resolve within 4 days of your period starting; you experience thoughts of self-harm in the premenstrual phase; symptoms are worsening over time; or lifestyle changes and OTC remedies haven't helped after 3 months. These may indicate PMDD, which requires specific treatment.
Sources: ACOG Practice Bulletin: Premenstrual Syndrome; Thys-Jacobs S. et al., Am J Obstet Gynecol 1998 (calcium RCT); Freeman EW et al., SSRI efficacy trials; Office on Women's Health (US Dept of Health & Human Services): Premenstrual Syndrome; Cleveland Clinic: PMS; Mayo Clinic: Premenstrual Syndrome — Symptoms and Causes; NIH/PubMed systematic reviews on PMS prevalence and treatment. This content is for informational purposes only. Always consult a qualified healthcare professional for diagnosis and treatment.

