
3–8%
Of reproductive-age women meet the clinical criteria for PMDD — about 62 million people globally
12–20 yrs
Average time between first symptoms and a correct PMDD diagnosis — one of the longest diagnostic delays in women's health
60–70%
Symptom reduction with first-line SSRI treatment — and many women respond within days, not weeks
In this article
- The key difference between PMS and PMDD
- Symptom comparison: what each one looks like
- When symptoms appear: the luteal phase explained
- The DSM-5 criteria: what doctors look for to diagnose PMDD
- PMDD vs depression vs anxiety: how to tell them apart
- Why PMDD takes so long to diagnose
- Effective treatments: medications, hormones, and lifestyle
- Supplements with clinical evidence
- How symptom tracking enables diagnosis
- When to see a doctor — and what to say
- Frequently asked questions
The key difference between PMS and PMDD
Almost every woman who menstruates experiences some premenstrual symptoms. Up to 75% of menstruating women report PMS — the bloating, mild irritability, breast tenderness, and fatigue that arrive in the week or so before a period. These symptoms are real, but they're manageable. You can push through them.
PMDD is categorically different. The primary driver of PMDD is not physical symptoms but severe emotional and psychological disruption — mood shifts so extreme that women describe feeling like a completely different person, relationships breaking down, being unable to get out of bed or go to work, and experiencing thoughts of suicide or self-harm. The cyclical lifting of these symptoms when the period arrives is often described as "coming back to myself." That dramatic difference — you before your period vs. you during your period — is one of the hallmarks of PMDD.
PMDD is listed in the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, 5th Edition) as a depressive disorder, which means it has a defined neurobiological basis, standardised diagnostic criteria, and qualifies for treatment and insurance coverage. It's not "bad PMS" — it's a distinct clinical entity that happens to be tied to the menstrual cycle.
The critical test: Do your symptoms — however severe — completely clear up within a few days of your period arriving? If you have a symptom-free window of at least 1–2 weeks after your period starts, that cycling pattern (not the severity alone) is the clearest indicator of PMDD over a persistent mood disorder.
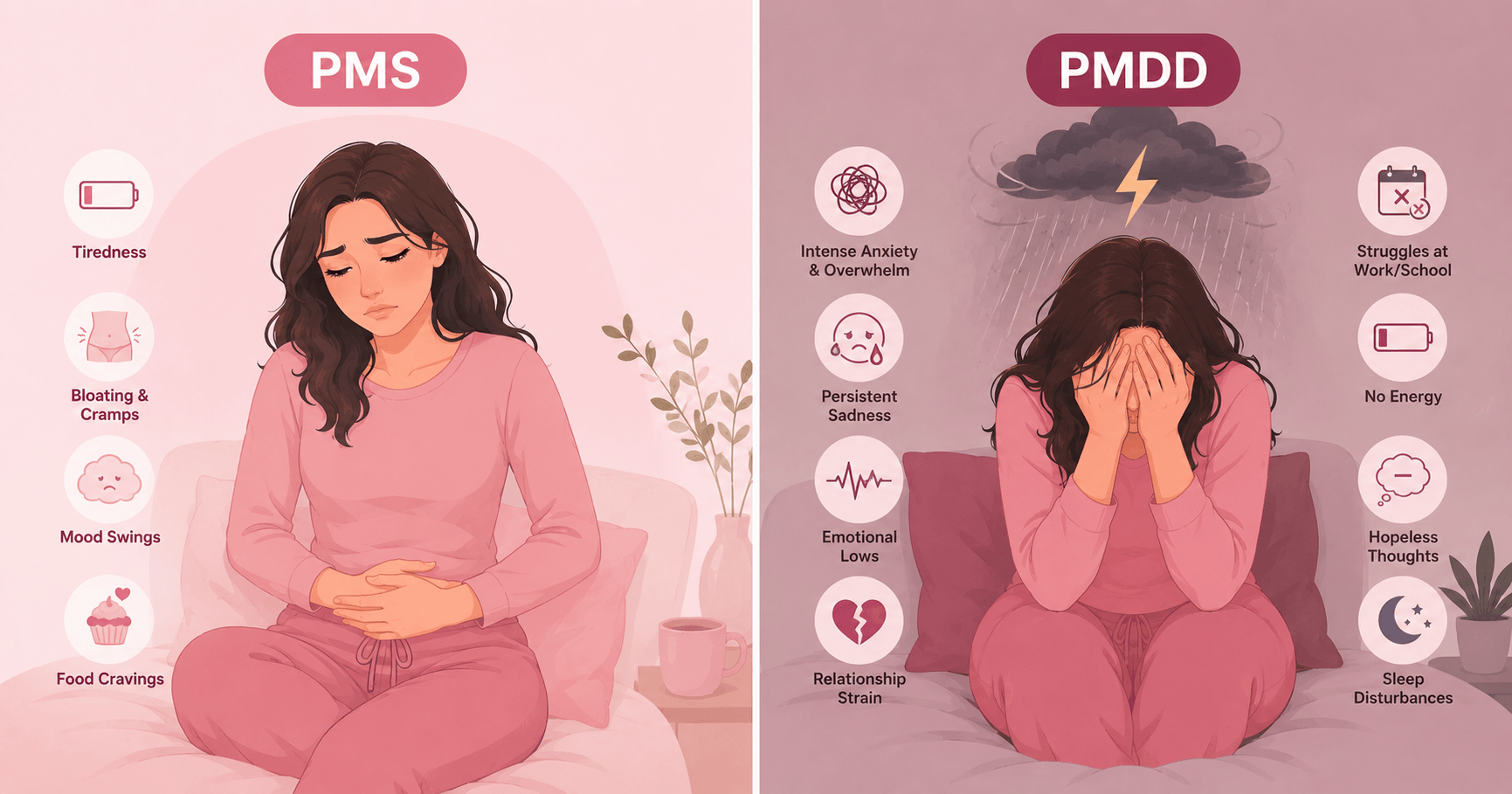
Symptom comparison: what each one looks like
Both PMS and PMDD share physical symptoms. The critical difference is in the emotional and behavioural domain — and in how much the symptoms interfere with your life.
| Symptom | PMS | PMDD |
|---|---|---|
| Mood changes | Mild irritability, tearfulness — uncomfortable but manageable | Severe mood swings, sudden rage, overwhelming sadness or hopelessness |
| Anxiety | Mild tension, feeling "on edge" in the day or two before period | Severe anxiety, panic, feeling out of control — can interfere with daily function |
| Depression | Low mood in the days before period | Profound hopelessness, self-deprecating thoughts, sometimes suicidal ideation |
| Irritability / anger | Short-tempered, snappy with others | Intense anger, conflicts that damage relationships, disproportionate reactions |
| Interest in daily life | Slightly reduced motivation | Marked withdrawal from work, social activities, hobbies — anhedonia |
| Concentration | Mild brain fog | Significant difficulty focusing — impacts work performance and decision-making |
| Energy / fatigue | Tiredness, feeling sluggish | Extreme lethargy, difficulty getting out of bed or leaving the house |
| Bloating | Noticeable but manageable | Often severe — a supporting symptom alongside the emotional criteria |
| Breast tenderness | Present, uncomfortable | Present — physical symptoms alone don't distinguish PMDD from PMS |
| Impact on daily life | Manageable — doesn't stop work or relationships | Clinically significant impairment — relationships, employment, or social functioning disrupted |
| Duration | Begins a few days before period, resolves quickly | Begins 1–2 weeks before period (luteal phase), resolves within a few days of onset |
Severity comparison across symptoms
PMS
PMDD
Mood / emotional symptoms
Anxiety / tension
Irritability / anger
Fatigue / low energy
Physical symptoms
Daily life disruption
When symptoms appear: the luteal phase explained
Both PMS and PMDD are strictly tied to the luteal phase — the second half of the menstrual cycle, from ovulation to the start of the next period. This cyclical pattern is what distinguishes them from persistent mood disorders like depression or anxiety, and understanding it is key to both recognising PMDD and documenting it for diagnosis.
28-Day Cycle: When PMS and PMDD Symptoms Appear
Menstruation
(Day 1–5)
(Day 1–5)
Follicular Phase
(Day 6–13) — SYMPTOM FREE
(Day 6–13) — SYMPTOM FREE
Ov.
Early Luteal
(Day 15–20) — mild symptoms
(Day 15–20) — mild symptoms
Late Luteal — PEAK SYMPTOMS
(Day 21–28)
(Day 21–28)
Symptom-free window (must exist for PMDD diagnosis)
Peak symptom phase — where PMDD is most severe
Ovulation (~Day 14)
Symptoms must be absent for at least 1 week after menstruation begins — this symptom-free window is essential to distinguish PMDD from a continuous mood disorder.
The cause of PMDD isn't elevated hormones — women with PMDD have normal estrogen and progesterone levels. The issue is an abnormal sensitivity to the normal hormonal fluctuations of the luteal phase, particularly the drop in estrogen and progesterone in the days before menstruation. This affects serotonin signalling in the brain, which explains why SSRIs — which target serotonin — are so effective for PMDD treatment.
The DSM-5 criteria: what doctors look for to diagnose PMDD
PMDD is diagnosed clinically — there is no blood test. Doctors use the DSM-5 criteria, which require at least 5 symptoms to be present during the luteal phase, with at least 1 core mood symptom among them, documented across at least 2 consecutive menstrual cycles.
DSM-5 PMDD Diagnostic Checklist
Core Mood Symptoms — at least 1 required
Marked affective lability — sudden mood shifts (e.g., feeling suddenly sad, tearful, or unusually sensitive to rejection)
Marked irritability or anger — increased interpersonal conflicts that feel out of proportion to the situation
Depressed mood — persistent low mood, hopelessness, or self-deprecating thoughts during the luteal phase
Marked anxiety or tension — feeling keyed up, on edge, or unusually anxious; not explained by other causes
Additional Symptoms — to reach total of 5
Decreased interest in usual activities (work, hobbies, socialising)
Difficulty concentrating or poor attention
Fatigue, lethargy, or markedly decreased energy
Change in appetite — overeating, food cravings, or loss of appetite
Sleep disturbance — insomnia or sleeping too much
Feeling overwhelmed or out of control
Physical symptoms — breast tenderness, bloating, muscle/joint pain, weight gain sensation
Timing requirement: Symptoms must be present only during the luteal phase and must remit within a few days of menstruation onset. A symptom-free follicular phase (after the period starts and before ovulation) is required. Symptoms must cause clinically significant distress or functional impairment in work, relationships, or daily activities. Must be confirmed across at least 2 consecutive cycles.
If you count 5 or more of the above symptoms (including at least 1 core mood symptom) that are specifically tied to your luteal phase and consistently disrupt your daily life, bring this checklist to your doctor. They may ask you to track symptoms prospectively for 2 months — a menstrual diary is the standard diagnostic tool.
PMDD vs depression vs anxiety: how to tell them apart
PMDD is the most commonly misdiagnosed condition in women's mental health — most often as major depression, bipolar disorder, or generalised anxiety disorder. The single most reliable distinguishing feature is cyclical timing.
PMDD
- Strictly cyclical — symptoms follow luteal phase
- Complete remission after period starts
- Symptom-free follicular phase (1–2 weeks minimum)
- Responds to luteal-phase-only SSRI dosing
- Responds to hormonal suppression
- Severity directly tied to ovulatory cycles
- Symptoms cease at menopause
Depression / Anxiety
- Persistent, continuous — not cycle-dependent
- Present throughout the month (may fluctuate)
- No consistent symptom-free window after period
- Requires continuous SSRI treatment
- Hormonal suppression doesn't resolve symptoms
- Not tied to ovulatory status
- Doesn't remit at menopause
Complicating this picture: PMDD and depression or anxiety can coexist. Women with PMDD have a higher lifetime risk of depression and anxiety, and existing mood disorders can be worsened during the luteal phase — a phenomenon called premenstrual exacerbation (PME). The key is determining whether the primary driver is cyclical (PMDD) or continuous (depression/anxiety) — which is why careful, consistent symptom tracking across the full cycle is essential for correct diagnosis.
Why PMDD takes so long to diagnose
The average PMDD diagnostic delay of 12–20 years isn't a failure of medicine alone — it's systemic. Women with PMDD see an average of 6 healthcare providers before receiving an accurate diagnosis, and are most often sent away with antidepressants for depression, mood stabilisers for "suspected bipolar," or reassurance that their symptoms are "just hormones."
Several factors contribute to this:
- Training gap: PMDD sits between psychiatry and gynaecology — neither specialty has historically owned it, so many doctors in both fields have minimal training in it.
- Symptom overlap: The emotional presentation of PMDD mimics depression and bipolar disorder precisely. Without cycle tracking data, distinguishing them is difficult.
- Gender bias in research: Women's cyclical symptoms have historically been dismissed or pathologised — "hysteria," "hormones," "overreacting." This culture persists in some clinical settings.
- Diagnostic requirement: PMDD requires 2+ months of prospective symptom tracking to confirm — most GP appointments don't allow time for this.
- Self-normalisation: Many women with PMDD have never had a symptom-free period to compare against — they've assumed severe premenstrual suffering is normal for everyone.
If you suspect PMDD, the single most useful thing you can do before your appointment is track your symptoms daily for 2 months, noting severity (1–10) and cycle day. This data can distinguish PMDD from depression in a way that a single consultation cannot, and transforms the appointment from an ambiguous conversation into a concrete clinical picture.
Effective treatments: medications, hormones, and lifestyle
PMDD has excellent treatment options — far better outcomes than many conditions with shorter diagnostic waits. The challenge is getting to diagnosis. Once there, a combination of approaches usually provides substantial relief.
SSRIs (First-Line Medication)
Fluoxetine (Sarafem), sertraline (Zoloft), and paroxetine CR (Paxil CR) are FDA-approved for PMDD. Importantly, women with PMDD often respond to lower doses than those used for depression, and some use luteal-phase-only dosing — taking the medication only in the 2 weeks before their period. Response can occur within days rather than the weeks required for depression.
First-line treatmentHormonal Contraceptives
Combined oral contraceptives containing drospirenone + ethinyl estradiol (brand names: Yaz, Beyaz) are FDA-approved for PMDD. They suppress ovulation, eliminating the luteal-phase hormonal fluctuations that trigger symptoms. Other combined pills, patches, and vaginal rings may also help, though with less PMDD-specific evidence.
FDA-approvedLifestyle Modifications
Regular aerobic exercise has strong evidence for mood regulation via endorphins and serotonin. Consistent sleep and wake times stabilise circadian rhythms that influence luteal-phase mood. Reducing caffeine, alcohol, and refined sugar during the luteal phase decreases anxiety and bloating. Stress management techniques and CBT (cognitive behavioural therapy) improve emotional regulation.
Strong support evidenceCBT & Psychological Support
Cognitive behavioural therapy helps women manage the emotional dysregulation of PMDD — not by dismissing symptoms as psychological, but by developing strategies to navigate the luteal phase without it destroying relationships and self-esteem. CBT works best alongside medical treatment for moderate-to-severe PMDD, and is especially valuable for managing the anticipatory anxiety of approaching the luteal phase.
Combined with medicationFor severe, treatment-resistant PMDD, GnRH agonists (gonadotropin-releasing hormone agonists) may be used to induce a temporary medical menopause, eliminating hormonal fluctuations entirely. This is typically a last resort before surgical menopause (oophorectomy) is considered, as GnRH agonists carry significant side effects.
If you are experiencing thoughts of suicide or self-harm: PMDD-related suicidal ideation is real and medically recognised. Please contact a crisis line immediately — in the UK call Samaritans: 116 123, in the US call or text 988 (Suicide & Crisis Lifeline). You deserve support, and effective treatment is available.
Supplements with clinical evidence
Several supplements have been tested in randomised controlled trials for PMDD and PMS. Calcium has by far the strongest evidence and should be the first non-prescription approach tried.
🥛 Calcium — 1,200 mg/day
Strong evidence
A double-blind RCT published in the American Journal of Obstetrics and Gynecology found that 1,200 mg of calcium carbonate daily reduced overall PMS/PMDD symptom scores by 48% compared to placebo. Benefits appeared within the first treatment cycle and continued improving over 3 months. Low calcium intake dysregulates calcium metabolism in the luteal phase, amplifying mood and physical symptoms.
🌿 Magnesium — 360 mg during luteal phase
Moderate evidence
Magnesium supplementation during the luteal phase reduces breast soreness, bloating, and mood symptoms in multiple trials, though evidence is less consistent than calcium. The luteal-phase-only approach (rather than continuous supplementation) mirrors the hormonal trigger window and avoids potential digestive side effects of daily high-dose magnesium.
🌱 Vitamin B6 — 50–100 mg/day
Moderate evidence
B6 is involved in serotonin and dopamine synthesis — the same neurotransmitter pathways disrupted in PMDD. A Cochrane review found B6 twice as likely to relieve overall premenstrual symptoms and depressive premenstrual symptoms compared to placebo. Do not exceed 100 mg/day without medical guidance, as higher doses can cause peripheral neuropathy with long-term use.
🌾 Chasteberry (Vitex agnus-castus)
Mixed evidence
Chasteberry acts on dopamine receptors and may reduce prolactin levels, which can decrease breast tenderness and irritability. Some trials show meaningful reduction in PMDD symptom scores; others show minimal effect over placebo. It appears most effective for physical symptoms (breast pain, bloating) rather than mood. Evidence for PMDD specifically is less robust than for general PMS.
How symptom tracking enables diagnosis
The DSM-5 requires prospective symptom documentation across at least 2 consecutive menstrual cycles to confirm PMDD. This isn't a bureaucratic hurdle — it's essential because it reveals the cyclical pattern that distinguishes PMDD from depression, and because retrospective self-reporting is notoriously inaccurate (we tend to either over-remember bad days or minimise them in hindsight).
1
Log symptoms daily — severity AND presence
Rate each symptom from 0 (absent) to 10 (severe) every day. Track: mood (depression, anxiety, irritability), physical symptoms (bloating, breast tenderness, fatigue), and functional impact (Did you miss work? Cancel plans? Have a significant conflict?). Daily logging is more accurate than weekly recall.
2
Record cycle day alongside symptoms
Knowing which day of your cycle you're on transforms raw symptom data into a diagnostic picture. A period-tracking app that auto-assigns cycle days removes this manual step. Two months of data showing symptoms consistently spiking in the luteal phase and clearing post-period is compelling clinical evidence.
3
Confirm a symptom-free window
One of the most diagnostic findings is the contrast. Document the days after your period when symptoms clear — the follicular phase symptom-free window. If you feel markedly better in the 1–2 weeks after your period starts, this cyclical pattern is a core PMDD indicator. If you're never symptom-free, that points toward a persistent mood disorder, possibly alongside PMDD.
4
Share the data with your doctor
Print or export your symptom log and bring it to your appointment. A clear visual of symptom timing across two cycles transforms the consultation from "I feel terrible before my period" (subjective, easily dismissed) to "Here is objective evidence of cyclical functional impairment" (clinical, actionable). This data is what gets referrals, diagnoses, and treatment.
Wamiga's daily symptom log tracks mood, energy, physical symptoms, and cycle day together — automatically generating the 2-cycle documented pattern your doctor needs to assess for PMDD. Download Wamiga free →
When to see a doctor — and what to say
You don't have to wait until symptoms are catastrophic. Any of the below warrants a doctor's appointment.
Symptoms are disrupting your work
Missing meetings, making errors, or needing sick days specifically in the week before your period — this is clinically significant functional impairment, one of the core PMDD criteria.
Relationships are being damaged
If your premenstrual irritability or mood swings are causing serious conflicts with partners, family, or colleagues that you later regret, this goes well beyond typical PMS and deserves investigation.
Thoughts of suicide or self-harm
Luteal-phase suicidal ideation is a recognised PMDD symptom. If you experience thoughts of not wanting to be here, self-harm, or hopelessness that remit after your period, tell your doctor this specifically — it escalates urgency appropriately.
Symptoms have worsened over time
PMDD can worsen with age, after hormonal events (pregnancy, contraception changes), or during perimenopause. Progressive worsening across cycles is a reason to seek assessment sooner rather than later.
What to say at the appointment: "I believe I may have PMDD. My mood, anxiety, and [specific symptoms] are severely disrupting my daily life in the 1–2 weeks before my period, and they completely resolve within a few days of my period starting. I've tracked this for two cycles and would like to discuss the DSM-5 criteria for PMDD." Bringing your tracking data makes this conversation far more productive. If your concerns are dismissed without discussion, seek a second opinion — this is a real, treatable condition.
Frequently asked questions
What is the main difference between PMS and PMDD?
The key difference is severity and functional impairment. PMS involves mild-to-moderate physical and mood symptoms that are uncomfortable but manageable. PMDD involves severe emotional symptoms — including marked depression, anxiety, and rage — that significantly interfere with work, relationships, and daily life. PMDD is a recognised clinical diagnosis in the DSM-5; PMS is not.
How do I know if I have PMDD and not just bad PMS?
Ask yourself two questions: (1) Are my symptoms severe enough to disrupt my work, relationships, or daily functioning? (2) Do my symptoms completely resolve within a few days of my period starting? If yes to both, PMDD is possible. Formal diagnosis requires tracking symptoms across at least 2 consecutive menstrual cycles and meeting at least 5 of the DSM-5 criteria, including at least 1 core mood symptom. See a doctor if you think you may have PMDD.
Is PMDD a mental illness?
Yes — PMDD is listed in the DSM-5 as a depressive disorder. This doesn't mean it's 'all in your head' — it means it has a recognised neurobiological basis involving abnormal sensitivity to normal hormonal fluctuations, particularly changes in progesterone and its effect on serotonin. The DSM-5 listing means it qualifies for treatment and insurance coverage.
How is PMDD different from depression?
The critical difference is timing. PMDD symptoms are strictly cyclical — they appear only in the luteal phase (1–2 weeks before menstruation) and completely disappear within a few days of your period starting. Depression is continuous and not tied to the menstrual cycle. If your lowest moods, anxiety, or irritability clear up completely for at least 1–2 weeks after your period arrives, that cyclical pattern points to PMDD rather than — or in addition to — depression.
What are the most effective treatments for PMDD?
First-line treatment is SSRIs. FDA-approved options include fluoxetine (Sarafem), sertraline (Zoloft), and paroxetine CR (Paxil CR). Women with PMDD often respond to lower doses than those used for depression, and some use luteal-phase-only dosing. Hormonal contraceptives containing drospirenone are also approved. Calcium (1,200 mg/day) has the strongest supplement evidence, showing ~48% symptom reduction in trials.
How common is PMDD?
PMDD affects approximately 3–8% of reproductive-age women globally — roughly 62 million people. It is significantly underdiagnosed, with studies showing an average diagnostic delay of 12–20 years and women seeing an average of 6 healthcare providers before receiving an accurate diagnosis. It is commonly misdiagnosed as major depression, bipolar disorder, or generalised anxiety disorder.
Can you treat PMDD without medication?
Yes — for mild-to-moderate PMDD, non-medication approaches can be effective. Calcium supplementation (1,200 mg daily) has the strongest evidence, with one RCT showing a 48% reduction in symptoms. Magnesium (360 mg during the luteal phase), regular aerobic exercise, reducing caffeine and alcohol, consistent sleep, and CBT can also provide meaningful relief. Medication is generally recommended for moderate-to-severe PMDD where quality of life is significantly impaired.
Sources: American Psychiatric Association DSM-5; ACOG Practice Bulletin on Premenstrual Syndrome; Thys-Jacobs S. et al. Am J Obstet Gynecol (calcium RCT); Oxford University Department of Psychiatry PMDD prevalence data; Cleveland Clinic: Premenstrual Dysphoric Disorder; NCBI/PMC systematic reviews on SSRI efficacy in PMDD; FDA-approved medication labelling (Sarafem, Yaz). This article is for informational purposes only. Always consult a qualified healthcare professional for diagnosis and treatment.