Day 21+
The threshold for "late" ovulation — anything after cycle day 21 in an average-length cycle
~22%
Per-cycle conception rate for women with late ovulation — comparable to the general average of ~21%
12–16 days
The luteal phase length — fixed regardless of when ovulation occurs, so late ovulation delays your period by the same amount
In this article
What is late ovulation?
Ovulation is triggered by a surge in luteinising hormone (LH), which causes a mature follicle in the ovary to rupture and release an egg. In a textbook 28-day cycle, this happens around day 14 — but real cycles aren't textbook. Normal ovulation occurs anywhere between cycle days 11 and 21, and cycle lengths of 21–35 days are all considered healthy.
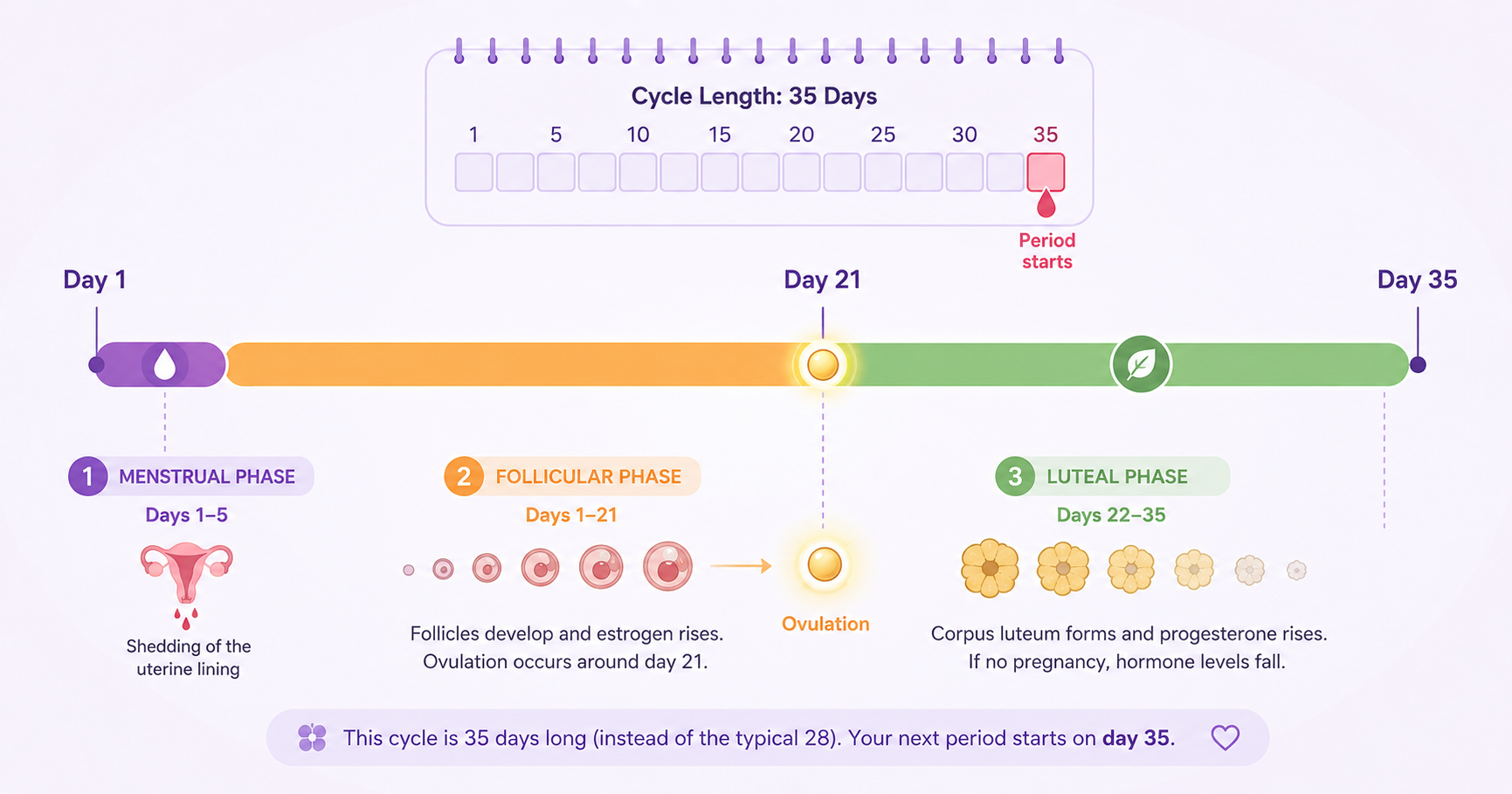
Late ovulation is generally defined as ovulation occurring after day 21 in a standard-length cycle, or significantly later than your established personal pattern. Because the luteal phase (ovulation to period) is relatively fixed at 12–16 days, late ovulation doesn't mean a late period is "irregular" — it means the follicular phase (period to ovulation) took longer than usual. Your period is simply arriving on schedule after a delayed egg release.
Key insight: Your cycle length is almost entirely determined by when you ovulate. The luteal phase rarely varies by more than 2–3 days. So if your cycles are 35–40 days, you're almost certainly ovulating around day 21–26 — not having a 40-day luteal phase. This is why calendar-based apps fail for late ovulators: they assume fixed ovulation on day 14.
7 causes of delayed ovulation
Late ovulation is almost always caused by something disrupting the hypothalamic-pituitary-ovarian (HPO) axis — the hormonal chain that times follicle development. Most causes are temporary and reversible.
Stress
The most common acute trigger. Cortisol directly suppresses GnRH pulsatility from the hypothalamus, delaying or blunting the LH surge. Even moderate life stress — exams, work pressure, relationship issues — can push ovulation 5–10 days later than usual in a single cycle.
Illness or fever
Any significant illness — flu, COVID-19, infection — can temporarily disrupt follicle development and delay ovulation during or in the cycle after the illness. The body deprioritises reproduction when fighting infection. This is a protective mechanism and typically resolves within 1–2 cycles.
PCOS
The most common chronic cause of late and irregular ovulation. Elevated androgens, high LH-to-FSH ratios, and insulin resistance disrupt normal follicle maturation, causing the body to repeatedly try and fail to trigger a surge before eventually succeeding — often much later than normal. Affects 6–12% of reproductive-age women.
Thyroid disorders
Both hypothyroidism (underactive) and hyperthyroidism (overactive) can delay ovulation by disrupting HPO axis signalling. Studies show ~24% of infertile women have hypothyroidism, and thyroid treatment restores regular ovulation in the majority. A TSH blood test is a simple first screen.
Significant weight change
Both rapid weight loss and weight gain disrupt hormonal signalling. In underweight women, low leptin levels suppress GnRH. In women with obesity, insulin resistance and elevated estrogen from fat tissue disrupt the HPO axis — creating a PCOS-like hormonal environment that delays ovulation.
Excessive exercise / low energy
High training volumes combined with insufficient caloric intake — common in athletes and runners — signal energy deficit to the hypothalamus. GnRH pulsatility decreases, LH surges become blunted and delayed. This form of hypothalamic suppression can cause progressively later ovulation before cycles stop entirely.
Stopping hormonal contraception
After stopping the pill, implant, patch, or hormonal IUD, the HPO axis needs time to re-establish its natural pulsatility. Most women resume ovulation within 1–3 cycles, but the first few cycles post-pill are often anovulatory or have delayed ovulation as hormone levels normalise.
Perimenopause
As the ovarian reserve declines from the late 30s onward, follicles respond more slowly to FSH signalling. The follicular phase progressively lengthens — meaning ovulation arrives later each year — before eventually cycles stop. This is a natural, expected transition, not a pathology.
How late ovulation shifts your period
The key rule: the luteal phase is fixed, the follicular phase is variable. Whatever day you ovulate, add 12–16 days to get your next period. This means every extra day of delay in ovulation pushes your period back by exactly the same number of days.
Day 1
Day 7
Day 14
Day 21
Day 28
Day 35
Day 42
Standard
cycle
cycle
Follicular (day 1–14)
Luteal (day 14–28)
Period: Day 28
Late
ovulation
ovulation
Follicular (day 1–21)
Luteal
Period: Day 35
Very late
ovulation
ovulation
Follicular (day 1–28)
Luteal
Period: Day 42
Follicular phase — varies
Luteal phase — fixed ~14 days
Ovulation point
This is why a "late period" is almost always actually "late ovulation." The uterine lining doesn't start its countdown until progesterone rises — which only happens after ovulation. A negative pregnancy test on what should have been day 28 does not mean something is wrong — it may simply mean ovulation hasn't happened yet, or just happened, and you are still in the two-week wait.
5 signs you're ovulating late
Consistently longer cycles (35+ days)
If your cycles are regularly 35–45 days, you're almost certainly ovulating late. The extra days are all in the follicular phase — your luteal phase is the same length as everyone else's. Track the pattern: consistent long cycles point to a structural cause (PCOS, thyroid); variable long cycles often point to lifestyle factors like stress.
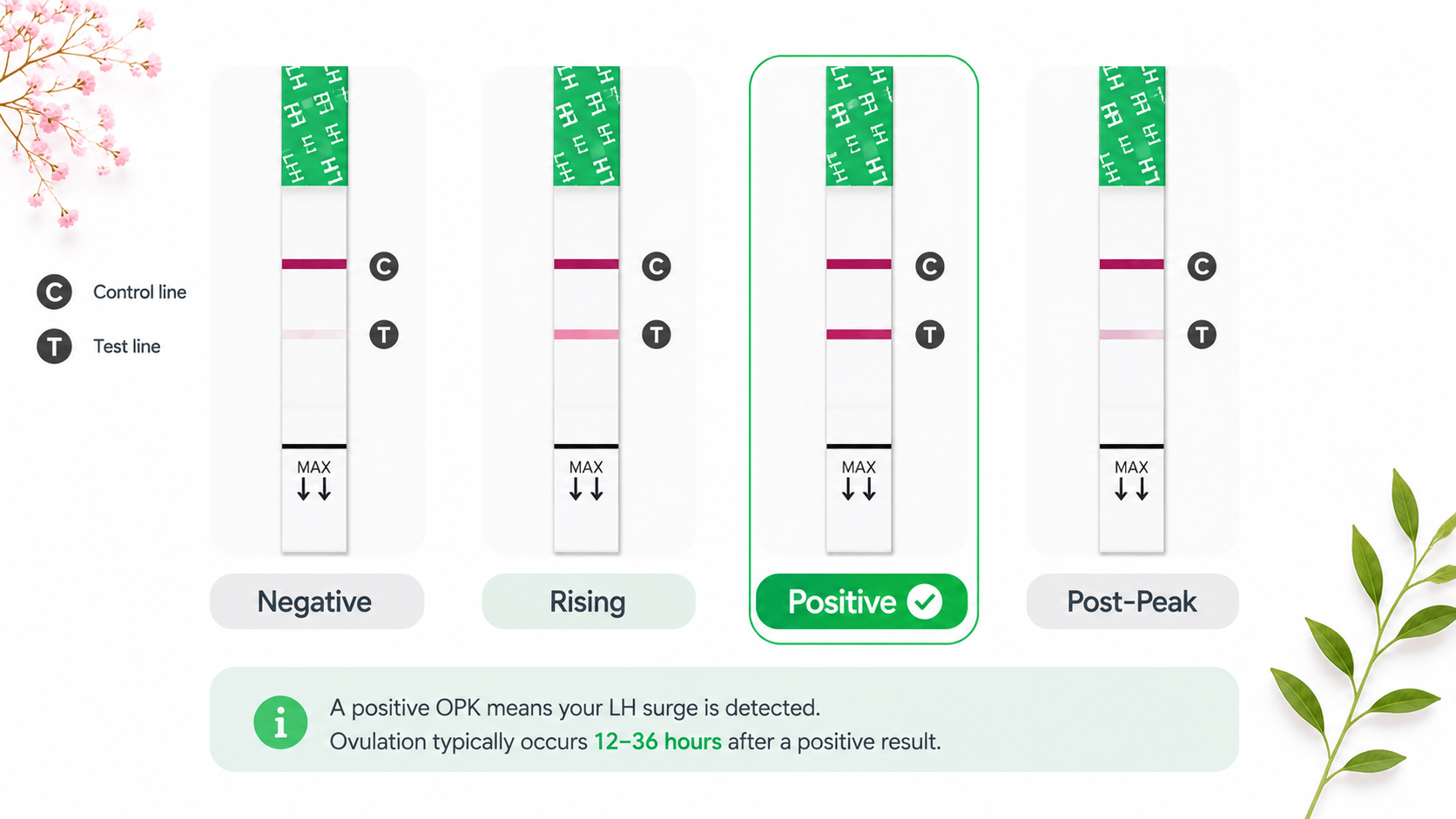
Positive OPK arriving after day 16
If you test daily and your LH surge doesn't appear until day 16, 20, or later, your body is taking longer than average to build up to ovulation. This is the clearest real-time indicator. Note that many apps and cycle calculators assume an LH surge around day 12–14 — they'll tell you to stop testing right when yours is about to begin.
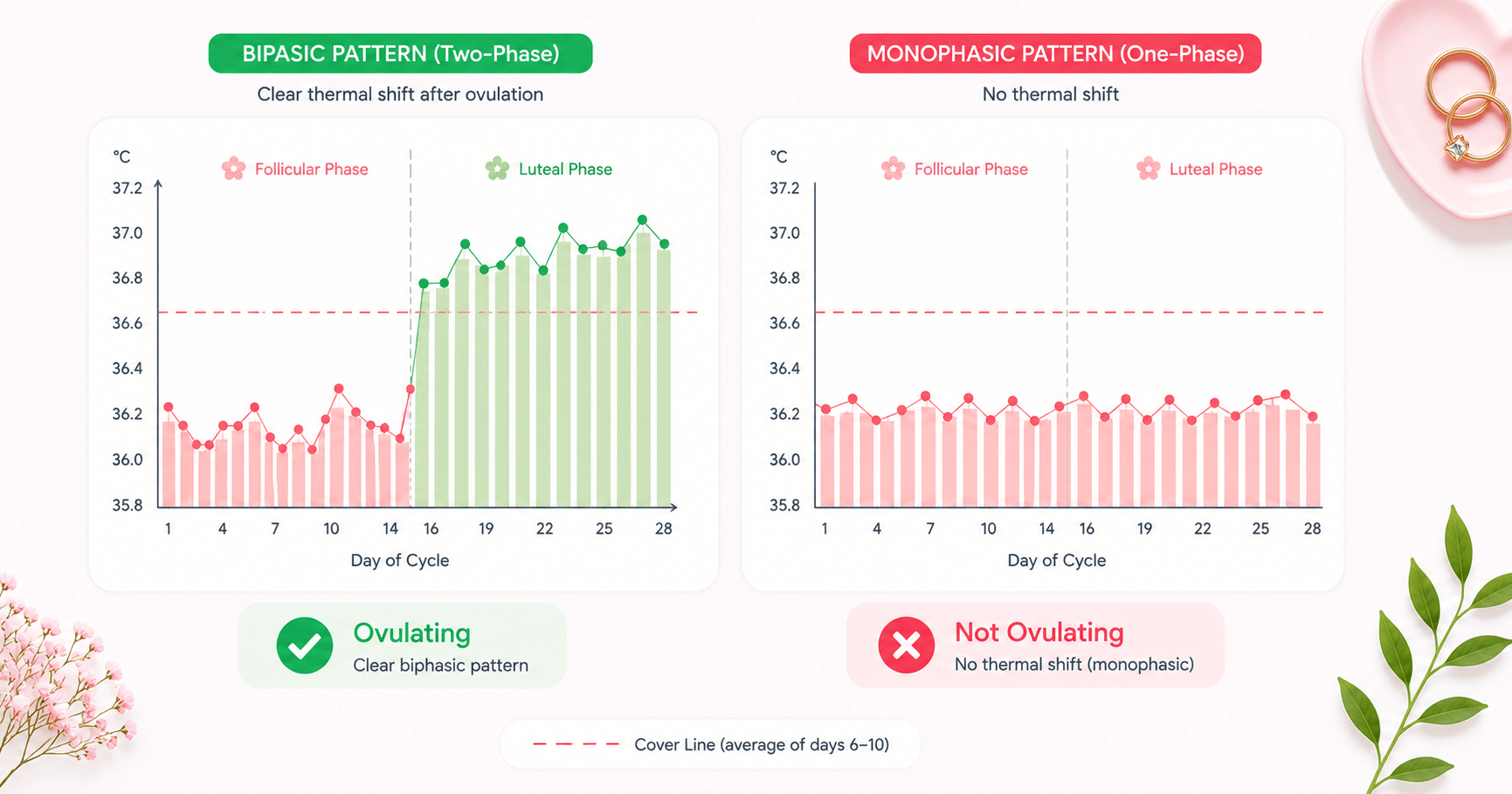
BBT thermal shift appearing late in the cycle
On your BBT chart, the clear rise from pre-ovulation temperatures will appear much later than expected — day 20, 22, 25, or even later. The chart will still show the same biphasic pattern; it just starts from a higher day number. If you've been expecting a shift around day 14 and stopping tracking around day 20, you may have been missing your actual thermal shift entirely.
Egg white cervical mucus (EWCM) appearing later than expected
Stretchy, clear, slippery cervical mucus is produced by rising estrogen in the days before ovulation. If you notice your EWCM arriving in week 3 or 4 of your cycle rather than week 2, your fertile window is simply shifted later. This mucus, whenever it appears, signals your optimal time for conception.
Mid-cycle pain or breast tenderness occurring later
If you usually notice brief ovulation cramps (mittelschmerz) or breast tenderness mid-cycle and these symptoms have been arriving in week 3 or 4, your ovulation has likely shifted later. Many women use the absence of these expected sensations in week 2 as a sign something is wrong — when in fact they're just waiting for an ovulation that arrives a week or two later.
How to track late ovulation — method comparison
Standard cycle-tracking advice is calibrated for "day 14 ovulation." If you ovulate late, you need to adapt your testing strategy — or you'll miss your fertile window entirely.
| Method | For Late Ovulators | Rating | Key Tip |
|---|---|---|---|
| OPK strips | Best overall — detects the LH surge 24–36 hours before ovulation, regardless of which day it occurs | Start testing from day 6 and continue until positive. Don't stop at day 14. | |
| BBT charting | Excellent for confirmation — the thermal shift will appear late but the pattern is identical to a normal cycle | Don't stop charting early. The shift may not appear until day 20–28. | |
| Cervical mucus | Good supporting evidence — EWCM appears close to your late LH surge. Combine with OPK for best results. | Monitor throughout — your EWCM will appear whenever you're approaching ovulation, not on a schedule. | |
| Calendar / period app | Unreliable — assumes fixed day 14 ovulation. Will consistently predict your fertile window 1–2 weeks too early. | Use only as a rough guide. Always combine with OPK or BBT confirmation. |
OPK testing window for late ovulators
Standard advice says to start OPK testing on day 9–10. Late ovulators need to start earlier and test longer — missing the surge because you stopped testing too early is one of the most common tracking mistakes in long-cycle women.
OPK Testing Windows — Standard vs Late Ovulation (28-day vs 35-day cycle)
Standard
(ovulates day 14)
(ovulates day 14)
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
Start day 9 ✓
Late ovulation
(ovulates day 21)
(ovulates day 21)
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
Start day 6 ✓
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
Not testing
Testing (negative)
LH surge (positive OPK)
Fertile window post-surge
Wamiga adapts its ovulation prediction to your actual cycle data — not a fixed day 14 assumption. After 2–3 cycles, it learns your personal ovulation window and reminds you to test at the right time. Download Wamiga free →
What late ovulation means for TTC
The most important thing to understand: late ovulation does not reduce your chance of conception per ovulatory cycle. Research shows per-cycle conception rates are comparable between women who ovulate late and the general population (~22% vs ~21%). The egg is viable, sperm can fertilise it, and implantation proceeds normally on the same DPO timeline.
Fertile window is still 5–6 days
The fertile window — the 5 days before ovulation plus the day of ovulation — remains unchanged in length. Sperm can survive 3–5 days in fertile cervical mucus. The window simply occurs later: around cycle days 16–21 rather than days 9–14 in typical late ovulators.
Fewer cycles per year
With 35–40 day cycles, you get 9–10 ovulatory cycles per year instead of 13. This reduces cumulative annual conception opportunities by ~25–30%. Over 12 months of trying, this is the primary practical impact — not a lower chance per cycle, but fewer attempts per year.
Timing from OPK matters more
Because calendar prediction fails, timing intercourse from actual OPK and cervical mucus data is essential. The optimal window is the 2 days before ovulation through ovulation day. Identify your LH surge, then aim for that day and the following 24 hours — the same as anyone TTC, just triggered by a later-arriving signal.
Egg quality is generally unaffected
A follicle that takes longer to mature does not automatically produce a lower-quality egg. Occasional late ovulation from lifestyle factors (stress, illness) has no meaningful impact on egg quality. Chronic late ovulation from PCOS or thyroid issues may affect egg quality in some cases, but this is linked to the underlying condition, not to the ovulation delay itself.
Luteal phase watch: In some women with late ovulation, the corpus luteum produces insufficient progesterone, leading to a luteal phase shorter than 10 days — called luteal phase insufficiency. This can prevent successful implantation. If you notice your period arriving fewer than 10 days after your confirmed BBT shift, mention this to your doctor.
When to take a pregnancy test with late ovulation
This is where late ovulators most commonly make mistakes: testing based on how many days since your last period rather than how many days since ovulation. Home urine tests detect hCG, which only starts rising after implantation — typically 6–10 days past ovulation (DPO). A reliable positive usually appears 12–14 DPO.
| Ovulation Day | Luteal Phase End | Reliable Urine Test From | What Cycle Day That Is |
|---|---|---|---|
| Day 14 (standard) | Day 28 | 12–14 DPO | Day 26–28 |
| Day 18 | Day 32 | 12–14 DPO | Day 30–32 |
| Day 21 | Day 35 | 12–14 DPO | Day 33–35 |
| Day 25 | Day 39 | 12–14 DPO | Day 37–39 |
| Day 28 | Day 42 | 12–14 DPO | Day 40–42 |
If you ovulated on day 25 and test on day 28 (when a standard cycle's period would be due), you are only 3 DPO — hCG hasn't even started rising yet. This is the most frequent reason late ovulators get confusing negative tests on days when they expect a period. Always count from your confirmed ovulation date, not from day 1.
When to see a doctor
1
Track for 3 cycles before drawing conclusions
A single cycle of late ovulation from stress, illness, or travel is very common and not medically significant. Track with OPKs and BBT for 3 complete cycles. If ovulation is consistently late (day 21+) across all three, or if cycles vary wildly from cycle to cycle, that's a pattern worth investigating.
2
Book a GP appointment if cycles are consistently over 35 days
Ask for a baseline hormone panel: FSH, LH, estradiol (day 2–5), mid-luteal progesterone (day 21 or 7 days after confirmed ovulation), TSH, prolactin, and AMH. This covers the most common causes — PCOS, thyroid disorders, hyperprolactinemia, and ovarian reserve — with a single blood draw.
3
See a specialist if TTC for 6+ months without success
If you've been trying to conceive for 6 months (over 35) or 12 months (under 35) with confirmed late ovulation, ask for a referral to a reproductive endocrinologist. PCOS-related late ovulation responds well to ovulation induction — letrozole achieves ovulation in ~70–80% of PCOS patients. Thyroid correction can restore regular ovulation quickly.
4
Act sooner if you have other symptoms
Don't wait if you also have: acne, excess facial or body hair, unexplained weight gain, scalp hair thinning (possible PCOS); fatigue, cold intolerance, hair loss, dry skin (possible hypothyroidism); milky nipple discharge outside breastfeeding (possible hyperprolactinemia). These warrant prompt investigation regardless of TTC status.
Frequently asked questions
What counts as late ovulation?
Late ovulation is generally defined as ovulation occurring after cycle day 21 in women with average-length cycles. However, 'late' is relative to your personal norm — if your cycles are consistently 35 days and you always ovulate around day 21, that's normal for you. The concern is when ovulation occurs much later than your established pattern, or when cycles exceed 35 days regularly.
Can you get pregnant with late ovulation?
Yes — late ovulation does not prevent conception. The fertile window simply occurs later in your cycle. Research shows women with late ovulation have conception rates of approximately 22% per cycle, comparable to the general population average of about 21%. Timing intercourse from your OPK surge or EWCM observation is effective regardless of what cycle day it occurs.
When should I take a pregnancy test if I ovulated late?
Count from your ovulation date, not from day 1 of your last period. A home urine pregnancy test becomes reliably positive 12–14 days past ovulation (DPO). If you ovulated on day 25 of your cycle, don't expect a positive until around day 37–39 — which would appear to be a very late period if you're counting from cycle day 1. Testing too early based on calendar date rather than ovulation date is the most common cause of false negatives in women with late ovulation.
Why is my ovulation getting later each cycle?
Progressively later ovulation across multiple cycles can indicate a developing hormonal issue worth investigating. Common causes include increasing stress, gradual weight changes, evolving thyroid dysfunction, or early perimenopause if you're in your late 30s to 40s. PCOS can also cause irregular, unpredictable ovulation timing that varies significantly cycle to cycle. A hormone blood panel (FSH, LH, TSH, prolactin, AMH) will identify the cause.
Does late ovulation cause a short luteal phase?
Not necessarily — the luteal phase is relatively fixed at 12–16 days regardless of when ovulation occurs. However, in some cases, late ovulation can be accompanied by a weaker corpus luteum and lower progesterone output, which may lead to a shorter or insufficient luteal phase. If your period arrives fewer than 10 days after a confirmed BBT thermal shift, it's worth discussing with a doctor.
Is late ovulation a sign of PCOS?
It can be. PCOS is the most common cause of chronically late or absent ovulation, affecting 6–12% of reproductive-age women. But late ovulation in isolation — especially after stress, illness, or lifestyle change — doesn't necessarily indicate PCOS. PCOS is typically associated with other signs including irregular periods, elevated androgens (acne, facial hair, scalp hair loss), and a characteristic polycystic ovary appearance on ultrasound.