~30%
Of female infertility cases are caused by anovulation or irregular ovulation
1–2/year
Anovulatory cycles per year that are considered normal even in fertile women
3 ng/mL
The minimum progesterone level on a day 21 blood test that confirms ovulation occurred
In this article
What is anovulation?
Your menstrual cycle is driven by a hormonal cascade: FSH triggers follicle growth, rising estrogen triggers an LH surge, and that LH surge causes the follicle to rupture and release an egg — ovulation. Anovulation occurs when this sequence breaks down before the egg is released. No egg means no corpus luteum, no progesterone production, and no fertile window that cycle.
What makes anovulation easy to miss is that it doesn't always stop bleeding. The uterine lining still builds up under estrogen, and when estrogen eventually drops, withdrawal bleeding occurs that can feel just like a period. This is called anovulatory bleeding — and it's the reason anovulation can go unnoticed for months or even years without cycle tracking.
Important distinction: A true menstrual period is triggered by falling progesterone after ovulation. Anovulatory bleeding is triggered by falling estrogen — it can look similar but has a completely different hormonal cause. An occasional anovulatory cycle (1–2 per year) is normal and not cause for alarm on its own.
8 signs you might not be ovulating
No single sign confirms anovulation on its own, but these are meaningful patterns worth tracking. The more of these you notice in the same cycle, the more worthwhile it becomes to investigate further.
1
No thermal shift on your BBT chart
After ovulation, progesterone causes your resting temperature to rise 0.2–0.5°C and stay elevated for the entire luteal phase. An anovulatory cycle produces a flat, monophasic chart — temperatures hover at roughly one level throughout, with no clear sustained rise above the cover line.
Strongest home indicator2
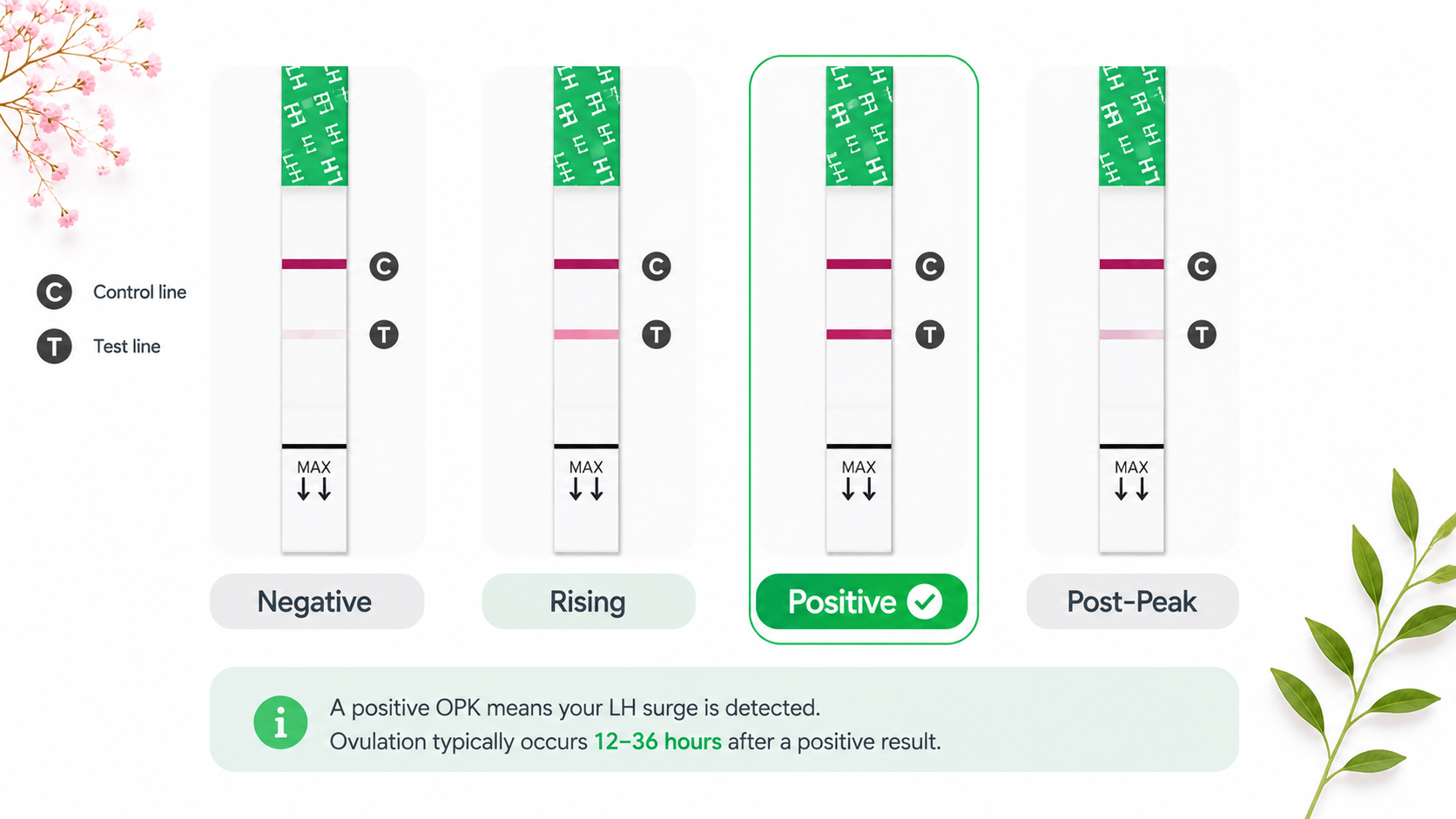
No positive OPK / LH surge detected
If you test daily from 5 days before expected ovulation and never see a positive OPK (test line equal to or darker than the control line), an LH surge — the hormonal trigger that causes the follicle to rupture — may not have occurred that cycle.
Strongly suggestive3
No egg white cervical mucus (EWCM)
Rising estrogen in the days before ovulation triggers clear, stretchy, slippery cervical mucus. If you track cervical mucus across a full cycle and never observe this fertile-quality mucus, follicular development may be absent or incomplete — no follicle, no estrogen surge, no EWCM.
Moderate indicator4
Irregular or very unpredictable cycles
Cycles consistently shorter than 21 days, longer than 35 days, or varying by more than 9 days from cycle to cycle often reflect irregular or absent ovulation. The follicular phase (before ovulation) is what varies most — in anovulatory cycles it can extend indefinitely while the body repeatedly tries and fails to trigger an LH surge.
Strongly suggestive5
No ovulation pain (mittelschmerz)
About 20–40% of ovulating women feel a brief one-sided twinge or cramp around ovulation caused by follicle rupture. If you've previously felt this mid-cycle sensation but it has now disappeared across multiple cycles, it may reflect an absence of follicle rupture — though many women who ovulate normally feel nothing at all.
Mild indicator6
Absent or very mild PMS symptoms
Classic PMS symptoms — breast tenderness, bloating, mood changes, fatigue — are driven by progesterone, the hormone produced only after ovulation by the corpus luteum. If your PMS has significantly reduced or disappeared in recent cycles, progesterone output may be low or absent.
Mild indicator7
Very light, irregular, or absent periods
Without ovulation, the uterine lining doesn't build up on a consistent schedule. This can produce very light spotting, skipped periods entirely, or irregular heavy bleeding if estrogen stays elevated for a prolonged time before dropping. Any major change in your bleeding pattern is worth noting.
Moderate indicator8
Short luteal phase (<10 days)
The luteal phase (ovulation to next period) is normally 12–16 days and is very consistent for each individual. A consistently short luteal phase — your period arriving fewer than 10 days after a BBT thermal shift — suggests inadequate progesterone production, which can indicate the quality of ovulation was poor even if it technically occurred.
Moderate indicatorWhat your BBT chart looks like without ovulation
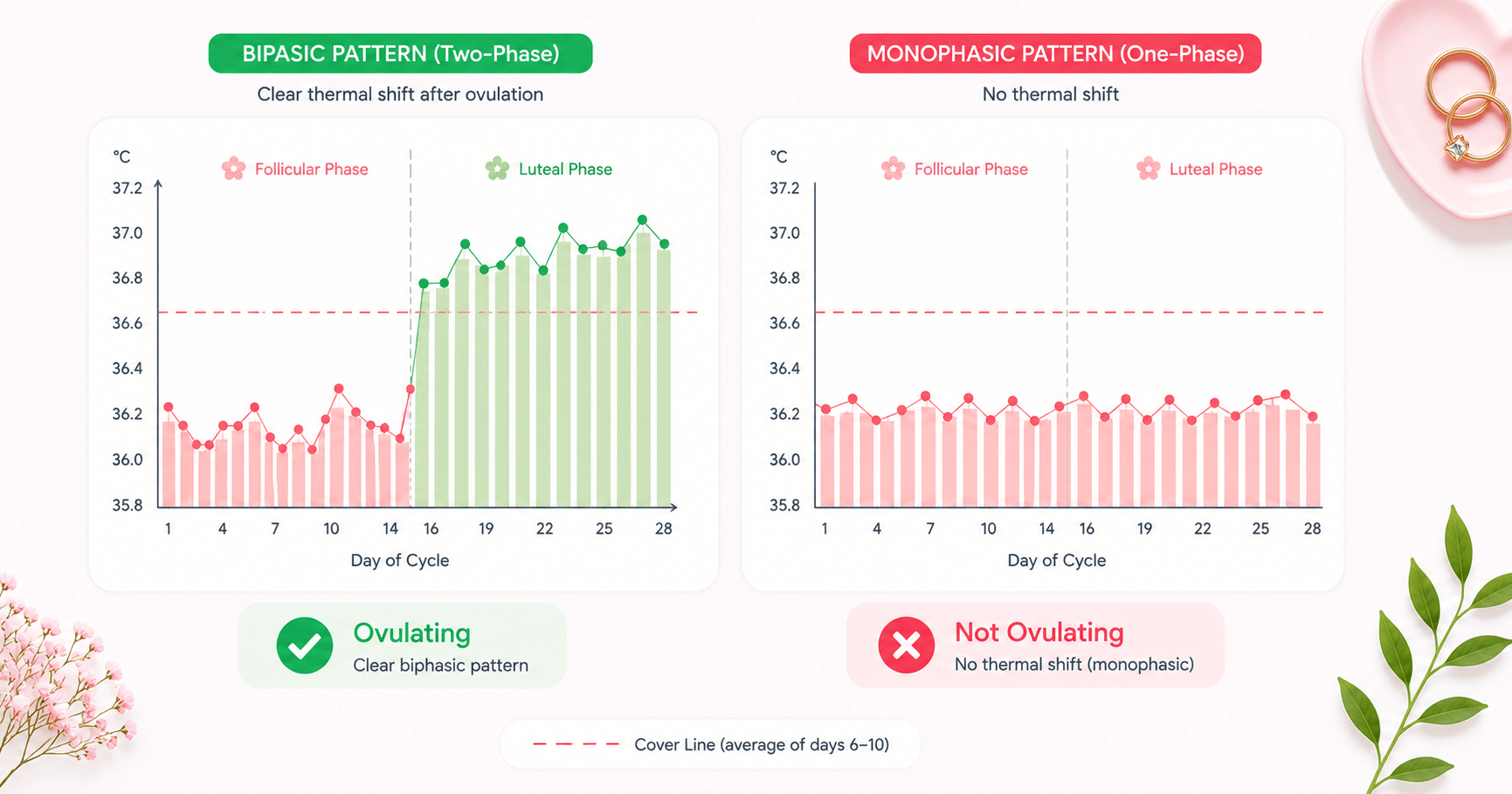
A BBT chart is the clearest at-home picture of whether ovulation has occurred. The difference between an ovulatory and anovulatory cycle is visible at a glance once you know the pattern.
Ovulatory Cycle — Biphasic Pattern
Temperature rises clearly after day 14 and stays elevated — confirming ovulation occurred. Two distinct phases visible.
Anovulatory Cycle — Monophasic Pattern
Temperatures fluctuate randomly but never sustain a clear rise. No second phase — no ovulation signal detected.
To draw a cover line: identify the highest temperature in your first 10 days of the cycle (pre-ovulation baseline), then draw a line 0.1°C above it. If 3 or more consecutive temperatures stay above that line, ovulation has been confirmed. In an anovulatory cycle, temperatures never achieve or sustain this pattern.
7 common causes of anovulation
Anovulation is almost always a symptom of an underlying hormonal disruption — not a standalone condition. Understanding the cause matters because treatment differs significantly for each.
1
PCOS (Polycystic Ovary Syndrome)
The most common cause of anovulatory infertility. Elevated androgens and LH, combined with insulin resistance in many cases, disrupt normal follicle development and prevent the LH surge needed for egg release. Affects ~10% of women of reproductive age.
~70% of anovulatory infertility — highly treatable with ovulation induction
2
Hypothalamic Amenorrhea (HA)
The hypothalamus suppresses GnRH release — and therefore FSH and LH — as a protective response to chronic energy deficit, excessive exercise, very low body weight, or prolonged psychological stress. Cycles may become irregular before stopping entirely.
~20% of cases — often fully reversible with lifestyle changes
3
Thyroid Disorders
Both hypothyroidism (underactive) and hyperthyroidism (overactive) disrupt the HPO axis controlling ovulation. Elevated TSH interferes with FSH and LH signalling. A simple blood test screens for this and treatment usually restores ovulation quickly.
Easily treatable once identified — often just thyroid hormone replacement
4
Hyperprolactinemia
Elevated prolactin (the hormone that promotes milk production) suppresses GnRH and inhibits ovulation. It can be caused by a small pituitary tumour (prolactinoma), certain medications (antipsychotics, antidepressants, blood pressure drugs), or hypothyroidism.
Treatable with dopamine agonist medication (cabergoline/bromocriptine)
5
Obesity and Insulin Resistance
Excess adipose tissue converts androgens to estrogen, creating a hormonal imbalance that disrupts the HPO axis. Elevated insulin drives excess androgen production and mimics the PCOS hormonal environment, disrupting follicle development and ovulation.
Weight loss of 5–10% can restore regular ovulation in many cases
6
Premature Ovarian Insufficiency (POI)
The ovaries stop functioning normally before age 40 — either the egg supply is depleted or the follicles stop responding to FSH. Cycles become increasingly irregular and anovulatory. Affects ~1 in 100 women under 40 and requires specialist management.
Requires referral to a reproductive endocrinologist
7
Perimenopause
As the ovarian reserve declines in the years before menopause (typically from the mid-40s onward), cycles become increasingly anovulatory. FSH rises as the ovaries respond less reliably to hormonal signals, and ovulation occurs in fewer and fewer cycles each year.
Expected and natural — anovulation increases progressively toward menopause
4 ways to confirm whether you're ovulating
Signs and symptoms are useful but not definitive. These four methods — from simplest and cheapest to most conclusive — will tell you with much greater certainty whether ovulation is occurring.
BBT Charting
Take your temperature every morning before getting up, at the same time (±30 min), using a BBT thermometer accurate to 0.01°C. A clear thermal shift of 0.2–0.5°C sustained for 3+ consecutive days confirms ovulation. Chart for 2–3 cycles to see your personal pattern clearly.
Free & at-homeOPK Testing
Test daily from 5 days before your expected ovulation date (day 9 for a 28-day cycle). A positive OPK — test line as dark as or darker than the control — confirms an LH surge has occurred. Consistently negative OPKs across 10+ days of testing suggests no surge that cycle.
At-home — highly sensitiveDay 21 Progesterone Blood Test
The gold standard for confirming ovulation. Blood drawn 7 days after suspected ovulation (day 21 in a 28-day cycle, or later if your cycle is longer) should show progesterone ≥3 ng/mL to confirm ovulation occurred. Levels ≥10 ng/mL suggest strong, adequate ovulation.
Gold standardFollicle Tracking Ultrasound
A series of transvaginal ultrasounds watches a follicle grow to mature size (~18–24mm), then confirms it has collapsed (ruptured) after the LH surge. This is the most direct visual confirmation of ovulation and is used routinely in fertility clinics for diagnosis and treatment monitoring.
Clinical — most directWamiga automatically detects your BBT cover line, marks the thermal shift on your chart, and flags cycles where no confirmed ovulation is detected — so you get clear answers without interpreting raw data yourself. Download Wamiga free →
What to do if you suspect anovulation
Work through these steps in order. Most causes of anovulation are identifiable within 1–2 months of tracking and a single blood draw.
Track for 2–3 complete cycles
One flat BBT chart can be caused by disrupted sleep, illness, or inconsistent wake times — it doesn't mean anovulation. Use both BBT charting and daily OPKs together. A consistent flat pattern across 2–3 cycles is meaningful; a single odd cycle usually isn't.
Address obvious lifestyle triggers first
Significant stress, undereating, excessive exercise, or rapid weight change are the most common and most reversible triggers. Reducing exercise intensity, increasing calorie intake, and managing chronic stress can restore ovulation within 2–3 months in most cases of hypothalamic amenorrhea — no medication required.
Request a basic hormone blood panel
Ask your GP for: FSH, LH, estradiol (days 2–5 of your cycle), mid-luteal progesterone (day 21 or 7 days after suspected ovulation), TSH, and prolactin. This covers the most common causes in a single blood draw and gives your doctor a clear picture to work from.
See a gynaecologist or reproductive endocrinologist
If blood work shows an abnormality, or if you've been trying to conceive for 6+ months with consistently anovulatory cycles, see a specialist. PCOS-related anovulation responds very well to ovulation induction — letrozole achieves ovulation in ~70–80% of patients, with strong cumulative conception rates.
Continue tracking during any treatment
Keep BBT charting and OPK testing throughout medical treatment. This tells both you and your doctor whether the intervention is working, helps time intercourse precisely during treatment cycles, and gives the data needed to adjust dosages if ovulation doesn't occur at the initial dose.
Frequently asked questions
Can you have a period without ovulating?
Yes. An anovulatory cycle can still produce bleeding that looks and feels like a period. Without ovulation, no progesterone is produced, so the estrogen-thickened uterine lining eventually breaks down and sheds — this is called anovulatory bleeding. It may be lighter, heavier, or more irregular than a true menstrual period.
What does an anovulatory cycle feel like?
An anovulatory cycle often feels subtly different: you may notice the absence of mid-cycle egg white cervical mucus, no mittelschmerz (ovulation pain), milder or absent PMS symptoms, and an irregular cycle length. Your BBT chart will show a flat, monophasic pattern with no thermal shift. However, some women notice no difference at all without tracking.
How do I know if my cycle is anovulatory?
The most reliable home method is BBT charting — an anovulatory cycle shows a monophasic (flat) chart with no sustained temperature rise. OPKs showing no LH surge across multiple days of testing also suggest anovulation. The definitive confirmation is a blood progesterone test taken 7 days after suspected ovulation (day 21 of a 28-day cycle) — a result below 3 ng/mL suggests ovulation did not occur.
Is it normal to occasionally not ovulate?
Yes — it's normal to have 1–2 anovulatory cycles per year, especially during periods of stress, illness, travel, or significant weight changes. The concern arises when anovulation becomes frequent or consistent across multiple cycles, as this can affect fertility and bone health due to the prolonged absence of progesterone.
What causes anovulation?
The most common cause is PCOS (polycystic ovary syndrome), which accounts for roughly 70% of anovulatory infertility. Other causes include hypothalamic amenorrhea (triggered by stress, low body weight, or over-exercise), thyroid disorders, elevated prolactin (hyperprolactinemia), premature ovarian insufficiency, obesity with insulin resistance, and perimenopause.
Can you get pregnant if you're not ovulating?
No — ovulation is required for natural conception. Without an egg being released, there is nothing for sperm to fertilize. If anovulation is causing fertility difficulties, effective medical treatments are available, including letrozole and clomiphene citrate, which successfully stimulate ovulation in the majority of women with PCOS.