~75%
Of menstruating people experience premenstrual symptoms — mood changes are among the most common
~5%
Have PMDD, a severe, diagnosable form where mood symptoms seriously disrupt daily life
Late luteal
The 5-day window before your period when mood swings peak — then lift as bleeding begins
In this article
- What period mood swings feel like (and are they normal?)
- Why they happen — the science, simply
- When in your cycle mood swings hit
- "Period rage" and period anxiety, explained
- PMS or PMDD? How to tell the difference
- How to cope — what actually works (ranked)
- Daily habits that steady your mood
- When to see a doctor
- Frequently asked questions
What period mood swings feel like — and are they normal?
Period mood swings are rapid, intense shifts in how you feel emotionally in the days before your period. They're not a character flaw or a sign you're "overreacting" — they're a physiological response to the steep hormonal changes of the luteal phase (the two weeks between ovulation and your period). Around 75% of menstruating people notice at least one premenstrual symptom each cycle, and emotional changes are some of the most frequently reported.
They show up differently for everyone, but the most common forms are:
Irritability & "period rage"
Small annoyances feel enormous. You snap at people you love, then feel guilty. A genuine, sudden anger that seems out of proportion.
Tearfulness & low mood
Crying at adverts, feeling flat or hopeless, or a sadness with no obvious trigger that lifts once your period starts.
Anxiety & tension
A wired, on-edge feeling, racing thoughts, or worry that's harder to switch off than usual — sometimes the most distressing symptom.
Emotional sensitivity
Feeling raw, easily overwhelmed, or like your emotional "volume" is turned up. Reactions feel bigger and harder to regulate.
This is considered a normal part of the cycle as long as the symptoms are mild-to-moderate, follow a clear pattern (after ovulation, easing within a few days of your period), and don't seriously damage your relationships or ability to function. When they cross that line into severe and disruptive, it may be PMDD — which we'll help you identify below.
Why period mood swings happen — the science, simply
Most articles stop at "your hormones change." That's true but incomplete. Here's the fuller picture — and the part that's genuinely reassuring.
Part 1: The estrogen–serotonin connection
Estrogen helps your brain produce and respond to serotonin, the neurotransmitter most responsible for stable mood, calm and emotional resilience. Estrogen peaks around ovulation, then falls through the luteal phase and dips again right before your period. As estrogen drops, serotonin activity drops with it — and a lower serotonin level means your threshold for irritability, sadness and anxiety is far easier to cross. Because serotonin also regulates sleep and appetite, this is why mood swings often arrive bundled with poor sleep and cravings.
Part 2: The missing piece — allopregnanolone and your brain's "calm switch"
After ovulation, progesterone rises and is converted into a neurosteroid called allopregnanolone (ALLO). ALLO acts on the GABA-A receptor — the same calming, anti-anxiety system that anti-anxiety medications target. In a stable system, this should make you feel calm. But two things go wrong in people prone to mood swings:
- Paradoxical response: In sensitive individuals, GABA-A receptors react to allopregnanolone in the opposite way — producing agitation, anxiety and irritability instead of calm.
- Withdrawal effect: In the late luteal phase, progesterone and allopregnanolone fall sharply right before bleeding. That rapid withdrawal destabilises the GABA system — much like the rebound effect of stopping a calming medication abruptly — heightening emotional reactivity at exactly the worst moment.
The reframe that changes everything
Research now shows that PMS and PMDD are not caused by abnormal hormone levels. Women with severe mood swings have the same hormone levels as everyone else. The difference is that their brains are more sensitive to the normal rise and fall of these hormones. Your hormones aren't broken — your brain is simply more responsive to a completely normal shift. That's why this isn't your fault, and why it's treatable.
When in your cycle do mood swings hit?
Period mood swings are cyclical by definition — that timing is actually the key diagnostic clue. They follow a predictable arc you can learn to anticipate.
Mood Stability Across a 28-Day Cycle
Period
Day 1–5
Lifting
Day 1–5
Lifting
Follicular — Most Stable
Day 6–14
Day 6–14
Ov.
Early Luteal
Day 15–22
Dipping
Day 15–22
Dipping
Late Luteal — MOOD LOW
Day 23–28
Day 23–28
Emotional steadiness
Most stable mood (follicular)
Mood begins dipping (early luteal)
Mood low point (late luteal)
Mood typically resets within 2–4 days of your period starting, as hormones reach their lowest, most stable point.
- Days 6–14 (Follicular): Rising estrogen supports serotonin. Most people feel their most emotionally stable, confident and resilient here.
- Days 15–22 (Early Luteal): Progesterone rises; mood begins a gradual decline. Mild sensitivity may appear.
- Days 23–28 (Late Luteal): Estrogen and serotonin drop while allopregnanolone withdraws. This is the peak for irritability, tearfulness and anxiety.
- Days 1–4 (Period): As bleeding starts, mood lifts and steadies — often noticeably within a day or two.
This predictability is your biggest advantage. If you know your low-mood window lands on days 24–28, you can avoid scheduling high-stakes conversations or stressful deadlines then, and build in extra rest and support — turning a blindside into a plan.
"Period rage" and period anxiety, explained
Two experiences deserve their own mention because they're so common yet rarely validated: period rage and period anxiety.
Period rage is the sudden, intense, almost out-of-body anger that can hit in the late luteal phase. It's not "just being moody" — falling serotonin reduces impulse control and emotional regulation, while the destabilised GABA system lowers your tolerance for frustration. Small triggers genuinely feel bigger because, neurologically, your brakes are weaker that week.
Period anxiety is the wired, on-edge, racing-thoughts feeling many people get premenstrually. It's directly linked to the allopregnanolone withdrawal effect on the GABA-A receptor — the same system that, when working normally, keeps anxiety in check. As that system wobbles, baseline anxiety rises, sometimes with physical symptoms like a racing heart or restlessness.
Naming these matters: they're recognised, mechanistic experiences — not personal failings — and the coping strategies below address both.
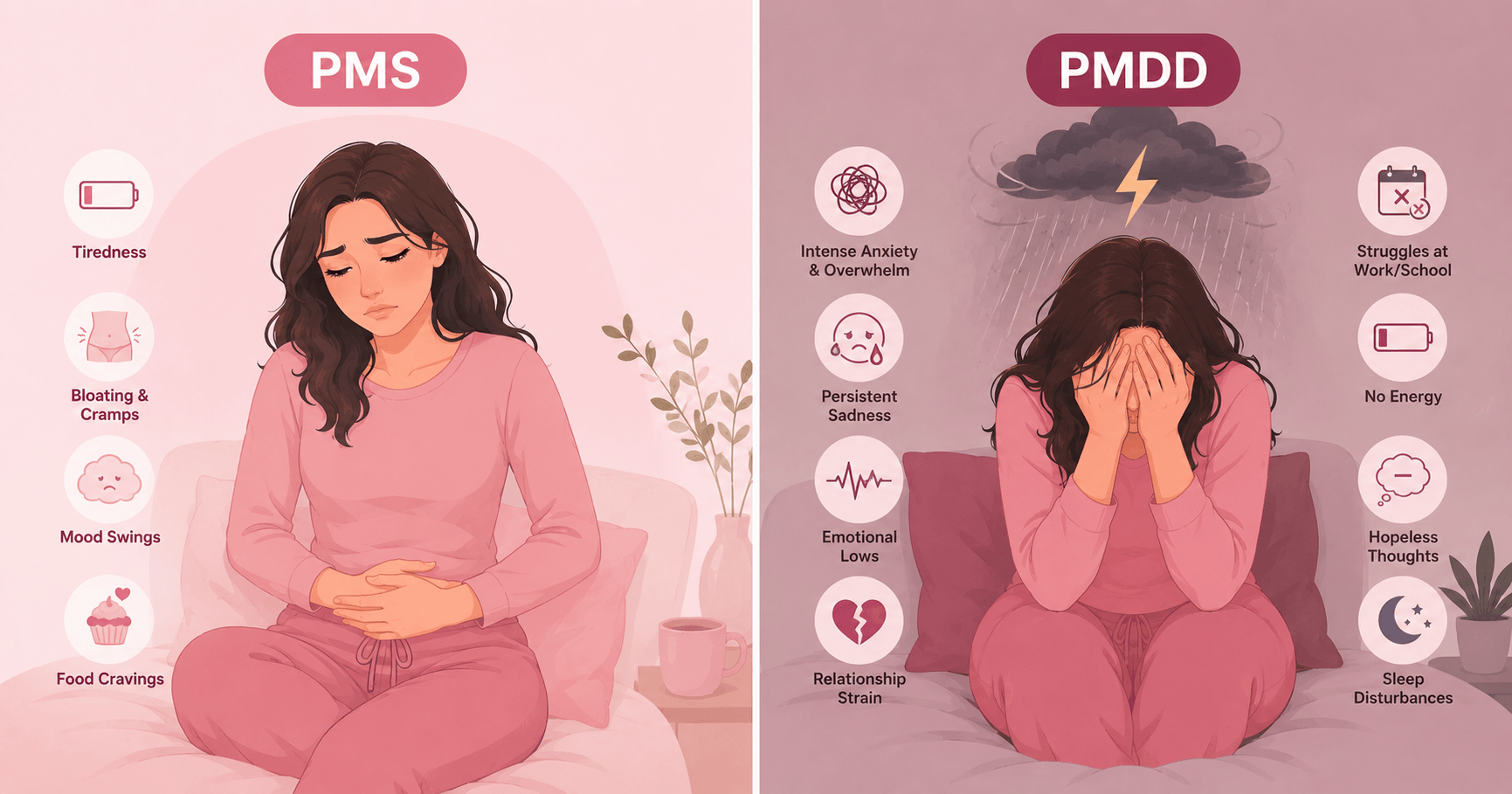
PMS or PMDD? How to tell the difference
The difference isn't the type of symptom — it's the severity and impact. PMS is annoying but manageable. PMDD is a severe, diagnosable condition (classified among depressive disorders) that can derail your life for one to two weeks of every month.
PMS (Premenstrual Syndrome)
PrevalenceUp to ~75%
SeverityMild–moderate
Daily lifeStill functional
Mood symptomsPresent, manageable
RelationshipsLargely intact
First-line helpLifestyle, tracking
PMDD (Dysphoric Disorder)
Prevalence~1.3–8%
SeveritySevere, disabling
Daily lifeSeriously impaired
Mood symptoms≥1 core, marked
RelationshipsOften damaged
First-line helpSSRIs / medical
Clinically, PMDD requires at least five symptoms in the week before your period, including at least one core emotional symptom — marked irritability or anger, depressed or hopeless mood, anxiety/tension, or pronounced mood swings — that significantly impair your functioning and resolve within a few days of menstruation. The single most reliable way to tell PMS and PMDD apart is to track your symptoms daily for two to three cycles: PMDD shows a stark, repeating premenstrual spike that lifts when your period arrives. For a deeper breakdown, see our PMS vs PMDD guide →
How to cope with period mood swings — what actually works
Here are the evidence-based options, ranked by how strong the research behind them is. Most people do best combining lifestyle foundations with one or two targeted additions — and, for severe symptoms, medical treatment.
🏃♀️ Regular aerobic exercise Strong
Raises serotonin and endorphins, lowers stress reactivity, and improves sleep — directly counteracting the luteal-phase mood dip. Aim for 30 minutes of moderate activity (brisk walking, swimming, cycling) most days. In the late luteal phase, favour moderate over high-intensity sessions, which can spike cortisol and worsen irritability.
💊 SSRIs (for severe PMS / PMDD) Strong — first-line
The first-line medical treatment for severe mood symptoms and PMDD. Uniquely, SSRIs (e.g. sertraline, fluoxetine) can work within days for PMDD — so some people take them only in the luteal phase rather than continuously. Highly effective but prescription-only: discuss with your doctor whether continuous or luteal-phase dosing suits you.
🥛 Calcium (~1,000–1,200 mg/day) Strong (best supplement)
The best-supported supplement for premenstrual mood. Randomised trials show calcium reduces mood symptoms, fatigue and cravings. Aim to get it from food first (dairy, fortified plant milks, leafy greens) and supplement the gap. Often paired with vitamin D for absorption.
🧠 CBT (cognitive behavioural therapy) Moderate–Good
Improves emotional regulation and reduces the impact of premenstrual depression and irritability. Works well on its own for milder cases and is additive with SSRIs for PMDD. Mindfulness-based approaches show similar benefits for the anxiety component.
💊 Combined hormonal contraception Moderate (individual)
Pills containing drospirenone can meaningfully reduce premenstrual mood symptoms for some by smoothing the hormonal fluctuation that triggers them. The catch: it's individual — some people feel better, others feel worse. Worth a monitored trial with your doctor if other options haven't helped.
🌿 Vitamin B6 (≤100 mg/day) & magnesium Mixed / supportive
Honest take: the evidence genuinely conflicts. B6 is a cofactor for serotonin synthesis and some reviews find it helps premenstrual mood, while others rate it insufficient as a first-line treatment — don't exceed 100 mg/day long-term. Magnesium has supportive but mixed evidence and may help the anxiety and sleep components. Both are low-risk to trial.
Tracking your mood daily in Wamiga — even a quick 1–5 rating alongside your cycle day — does two things at once: it confirms whether your symptoms are truly cyclical (the actual basis for a PMDD diagnosis) and it predicts your low-mood days so you can prepare. After 2–3 cycles, the pattern is clear enough to plan around. Download Wamiga free →
Daily habits that steady your mood
Do more of this
- Protein + complex carbs together — steadies blood sugar; swings worsen irritability
- Consistent sleep schedule — poor sleep amplifies every mood symptom
- Daily movement — even a 20-minute walk lifts serotonin
- 10 min of breathing / mindfulness — measurably lowers cortisol over 2–3 cycles
- Tryptophan-rich foods (eggs, turkey, oats, pumpkin seeds) — serotonin building blocks
- Plan light weeks around your low window — protect your energy in the late luteal phase
Ease off this premenstrually
- Alcohol — disrupts sleep and worsens low mood and anxiety
- Excess caffeine — amplifies anxiety and the on-edge feeling
- Refined sugar & skipped meals — blood-sugar crashes magnify irritability
- Over-scheduling — high-stakes stress lands hardest in the late luteal phase
- Doom-scrolling before bed — the luteal brain is more reactive to poor sleep
- Self-criticism — this is biology, not a flaw; treat yourself accordingly
When to see a doctor about premenstrual mood changes
Period mood swings are common, but some patterns deserve professional support.
Symptoms are severe and follow a clear premenstrual pattern
If marked irritability, depression or anxiety appears in the ~5 days before your period for at least three consecutive cycles and ends within a few days of bleeding — and it's disrupting work or relationships — that pattern fits PMDD and is highly treatable. Bring a 2–3 cycle symptom log to your appointment.
Your mood doesn't lift once your period starts
True PMS/PMDD resolves within a few days of menstruation. If low mood or anxiety is present all month and merely worsens premenstrually, that can signal an underlying depression or anxiety disorder (or "premenstrual exacerbation" of one) that needs its own treatment.
It's straining your relationships or quality of life
You don't have to meet a formal threshold to deserve help. If premenstrual mood changes are hurting your relationships, work or wellbeing, that alone is a good reason to talk to a clinician about lifestyle, therapy and medical options.
Please don't wait if it's urgent. If you ever have thoughts of harming yourself or that life isn't worth living — even if only premenstrually — seek help immediately. Contact a crisis line, your doctor, or your local emergency services. In the US you can call or text 988; in the UK call 111 or the Samaritans on 116 123. These feelings are a treatable symptom, not the truth about you.
Frequently asked questions
Why do I get mood swings before my period?
They're driven by the hormone shifts of the luteal phase. Falling estrogen reduces serotonin (your mood-stabilising neurotransmitter), while the sharp withdrawal of progesterone's metabolite allopregnanolone destabilises your brain's GABA "calm" system right before your period. In sensitive people this amplifies irritability, tearfulness and anxiety. Importantly, this reflects a brain that's more sensitive to normal hormone changes — not abnormal hormones.
Are period mood swings normal?
Yes — up to 75% of menstruating people experience premenstrual symptoms, and mood changes are among the most common. They're considered normal when mild-to-moderate, clearly patterned (after ovulation, easing within a few days of your period), and not seriously disrupting your life. Severe, disabling mood symptoms may be PMDD and are worth discussing with a doctor.
How long do period mood swings last?
They usually begin in the luteal phase after ovulation (around days 15–22 of a 28-day cycle), peak in the final 5 days before your period, and lift within 2–4 days of bleeding starting. If your low mood doesn't clear once your period arrives — or is present all month and just worsens premenstrually — that points to an underlying mood condition rather than PMS and is worth evaluating.
What hormone causes mood swings before a period?
It's an interaction, not one hormone. Falling estrogen lowers serotonin activity, and progesterone's metabolite allopregnanolone destabilises the GABA-A "calm" system as it withdraws before your period. Serotonin, dopamine and cortisol all contribute. The key finding from recent research is that people with PMS/PMDD have normal hormone levels — their brains are simply more sensitive to the normal rise and fall.
Is it PMS or PMDD — how do I tell the difference?
PMS is mild-to-moderate and manageable; PMDD is severe and disabling, affecting roughly 1.3–8% of menstruating people. PMDD requires at least five symptoms in the week before menses with at least one core emotional symptom (marked irritability/anger, depressed mood, anxiety, or mood swings) that significantly impair functioning and resolve within days of your period. The best way to distinguish them is to track symptoms daily for 2–3 cycles to confirm the repeating premenstrual spike.
How do I stop period mood swings naturally?
The best-evidenced natural strategies are regular aerobic exercise, calcium (~1,000–1,200 mg/day), consistent quality sleep, stress reduction via CBT or mindfulness, and stable blood sugar from protein-rich meals. Easing off alcohol, caffeine and refined sugar premenstrually helps many people, and vitamin B6 (≤100 mg/day) and magnesium have supportive but mixed evidence. Tracking your cycle to anticipate low-mood days is one of the most practical tools. For severe symptoms, SSRIs and certain hormonal contraceptives are highly effective — talk to your doctor.
Sources: Office on Women's Health — Premenstrual Syndrome; NHS — Premenstrual Syndrome (PMS); AAFP — PMS and PMDD (diagnostic criteria, prevalence, treatment evidence grades); ACOG — Premenstrual Dysphoric Disorder; Mayo Clinic — PMS symptoms & causes; Frontiers in Psychiatry (2023) and ScienceDirect — allopregnanolone and GABA-A receptor sensitivity in PMDD. Content is for informational purposes only — consult a qualified healthcare professional for diagnosis and treatment.